Developmental Evaluation of Infants Who Have Received Tadalafil in Utero for Fetal Growth Restriction

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Maki, S.; Tanaka, H.; Tsuji, M.; Furuhashi, F.; Magawa, S.; Kaneda, M.K.; Nii, M.; Tanaka, K.; Kondo, E.; Tamaru, S.; et al. Safety evaluation of tadalafil treatment for fetuses with early-onset growth restriction (TADAFER): Results from the Phase II trial. J. Clin. Med. 2019, 8, 856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharp, A.; Conforth, C.; Jackson, R.; Harrold, J.; Turner, M.A.; Kenny, L.C.; Baker, P.N.; Johnstone, E.D.; Khalil, A.; von Dadelszen, P.; et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): A multicenter, randomized, placebo-controlled, double-blind trial. Lancet Child. Adolesc. Health 2018, 2, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Groom, K.; Ganzevoot, W.; Alfirevic, Z.; Lim, K.; Papageorghiou, A.T. STRIDER Consortium. Clinicians should stop prescribing sildenafil for fetal growth restriction (FGR): Comment from the STRIDER Consortium. Ultrasound Obstet. Gynecol. 2018, 52, 295–296. [Google Scholar] [CrossRef] [Green Version]
- Kubo, M.; Umekawa, T.; Maekawa, Y.; Tanaka, H.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Ikeda, T. Retrospective study of tadalafil for fetal growth restriction: Impact on maternal and perinatal outcomes. J. Obstet. Gynaecol. Res. 2017, 43, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Tanaka, H.; Maki, S.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Umekawa, T.; Kondo, E.; Ikeda, T. Safety and dose-finding trial of tadalafil administered for fetal growth restriction: A phase-1 clinical study. J. Obstet. Gynaecol. Res. 2017, 43, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Leppänen, M.; Lapinleimu, H.; Lind, A.; Matomäki, J.; Lehtonen, L.; Haataja, L.; Päivi, R. Antenatal and postnatal growth and 5-year cognitive outcome in very preterm infants. Pediatrics 2014, 133, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Guellec, I.; Lapillonne, A.; Marret, S.; Picaud, J.C.; Mitanchez, D.; Charkaluk, M.L.; Mitanchez, D.; Charkaluk, M.L.; Fresson, J.; Arnaud, C.; et al. Effect of intra- and extrauterine growth on long-term neurologic outcomes of very preterm infants. J. Pediatr. 2016, 175, 93–99. [Google Scholar] [CrossRef]
- Takeuchi, A.; Yorifuji, T.; Nakamura, K.; Tamai, K.; Mori, S.; Nakamura, M.; Kageyama, M.; Kubo, T.; Ogino, T.; Kobayashi, K.; et al. Catch-up growth and neurobehavioral development among full-term, small-for-gestational-age children: A nationwide japanese population-based study. J. Pediatr. 2018, 192, 41–46. [Google Scholar] [CrossRef]
- Society for the Kyoto Scale of Psychological Development Test. Shinpan K Shiki Hattatsu Kensahou 2001 Nenban [The Kyoto Scale of Psychological Development Test 2001]; Nakanishiya Shuppan: Kyoto, Japan, 2008. (In Japanese) [Google Scholar]
- Dunn, L.; Greer, R.; Flenady, V.; Kumar, S. Sildenafil in Pregnancy: Systematic Review of Maternal Tolerance and Obstetric and Perinatal Outcomes. Fetal Diagn. Ther. 2017, 41, 81–88. [Google Scholar] [CrossRef]
- Kono, Y.; Yonemoto, N.; Kusuda, S.; Hirano, S. Developmental assessment of VLBW infants at 18 months of age: A comparison study between KSPD and Bayley III. Brain Dev. 2015, 10, 10. [Google Scholar]
- Kunihiko, N.; Toru, H.; Tomoko, S.; Nakai, K.; Hosokawa, T.; Satoh, H. Comparison of Kyoto Scale of Psychological Development and Bayley Scales of Infant Development second edition among japanese infants. J. Spec. Educ. Res. 2013, 2, 17–24. [Google Scholar]
- Miller, S.L.; Huppi, P.S.; Mallard, C. The consequences of fetal growth restriction on brain structure and neurodevelopmental outcome. J. Physiol. 2016, 594, 807–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, E. Paediatric implications of IUGR with special reference to cerebral palsy. In Intrauterine Growth Restriction Aetiology and Management; Kingdom, J., Baker, P., Eds.; Springer: London, UK, 2000; pp. 351–366. [Google Scholar]
- Marlow, N. Paediatric implications–neonatal complications. In Intrauterine Growth Restriction Aetiology and Management; Kingdom, J., Baker, P., Eds.; Springer: London, UK, 2000; pp. 337–349. [Google Scholar]
- Gagnon, R. Placental insufficiency and its consequences. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 110, S99–S107. [Google Scholar] [CrossRef]
- Yanney, M.; Marlow, N. Paediatric consequences of fetal growth restriction. Semin. Fetal. Neonatal Med. 2004, 9, 411–418. [Google Scholar] [CrossRef] [PubMed]
- van Wassenaer, A. Neurodevelopmental consequences of being born SGA. Pediatr. Endocrinol. Rev. 2005, 2, 372–377. [Google Scholar] [PubMed]
- Guellec, I.; Lapillonne, A.; Renolleau, S.; Charlaluk, M.L.; Roze, J.C.; Marret, S.; Vieux, R.; Monique, K.; Ancel, P.Y.; Group, E.S. Neurologic outcomes at school age in very preterm infants born with severe or mild growth restriction. Pediatrics 2011, 127, 883–891. [Google Scholar] [CrossRef]
- von Beckerath, A.K.; Kollmann, M.; Rotky-Fast, C.; Karpf, E.; Lang, U.; Klaritsch, P. Perinatal complications and long-term neurodevelopmental outcome of infants with intrauterine growth restriction. Am. J. Obstet. Gynecol. 2013, 208, 130.e1–130.e6. [Google Scholar] [CrossRef]
- Low, J.A.; Handley-Derry, M.H.; Burke, S.O.; Peters, R.D.; Pater, E.A.; Killen, H.L.; Derrick, E.J. Association of intrauterine fetal growth retardation and learning deficits at age 9 to 11 years. Am. J. Obstet. Gynecol. 1992, 167, 1499–1505. [Google Scholar] [CrossRef]
- Kok, J.H.; den Ouden, A.L.; Verloove-Vanhorick, S.P.; Brand, R. Outcome of very preterm small for gestational age infants: The first nine years of life. Br. J. Obstet. Gynaecol. 1998, 105, 162–168. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Fattal-Valevski, A.; Harel, S. Memory functions of children born with asymmetric intrauterine growth restriction. Brain Res. 2006, 1117, 186–194. [Google Scholar] [CrossRef]
- Geva, R.; Eshel, R.; Leitner, Y.; Valevski, A.F.; Harel, S. Neuropsychological outcome of children with intrauterine growth restriction: A 9-year prospective study. Pediatrics 2006, 118, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Fischi-Gomez, E.; Vasung, L.; Meskaldji, D.E.; Lazeyras, F.; Borradori-Tolsa, C.; Hagmann, P.; Barisnikov, K.; Thiran, P.; Huppi, P.S. Structural brain connectivity in school-age preterm infants provides evidence for impaired networks relevant for higher order cognitive skills and social cognition. Cereb. Cortex 2014, 25, 2793–2805. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Tadalafil Dose | ||||
|---|---|---|---|---|
| 10 mg | 20 mg | 40 mg | Total | |
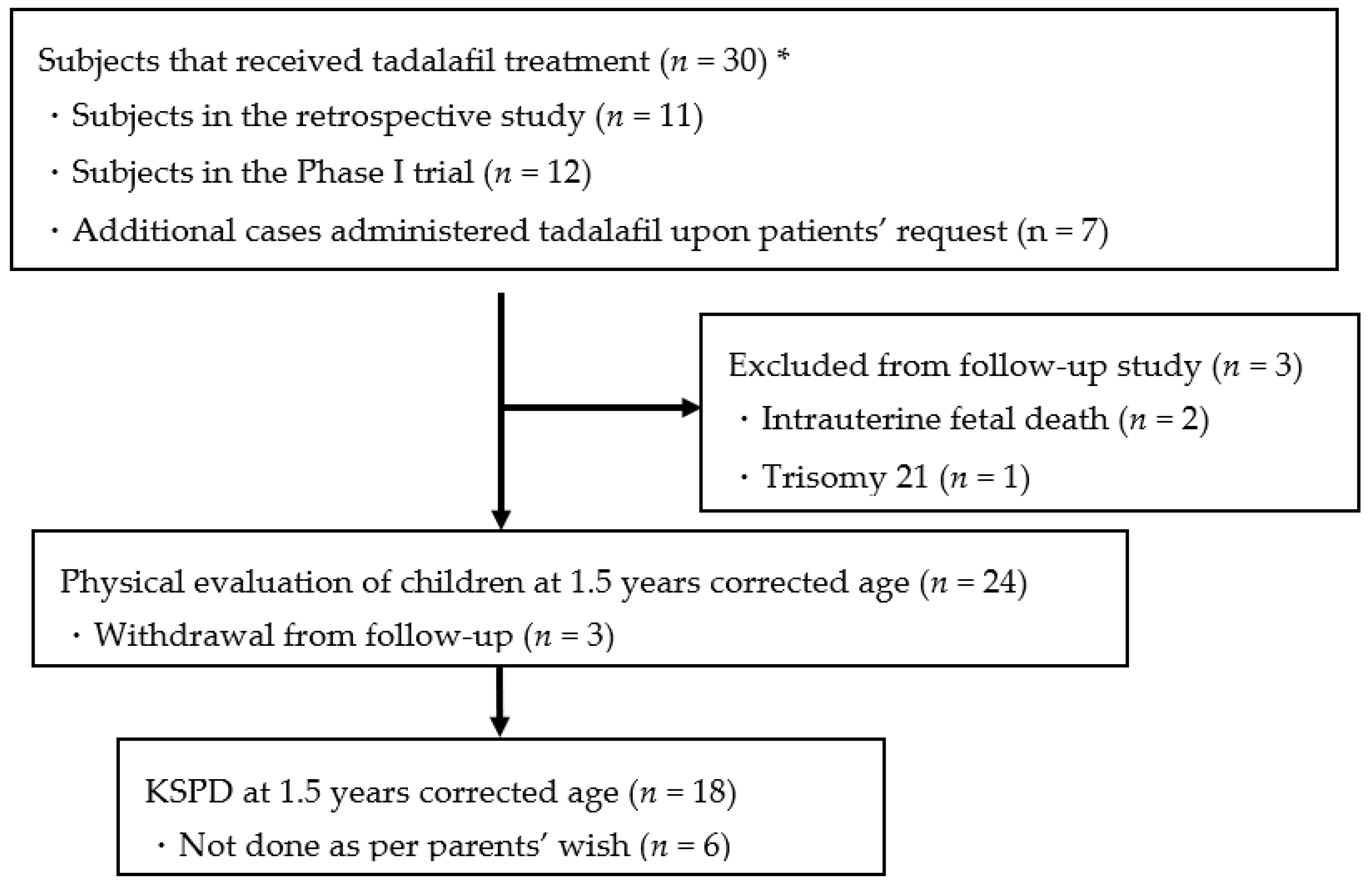
| Total number of cases administered tadalafil | 3 | 20 | 7 | 30 |
| Intrauterine fetal death | 1 | 1 | 2 | |
| Trisomy 21 | 1 | |||
| Withdrawal from follow-up | 2 | 1 | 3 | |
| Number of follow-up cases (at least 1.5 years corrected age) | 3 | 16 | 5 | 24 |
| KSPD at 1.5 years corrected age) | 2 | 11 | 5 | 18 |
| N = 24 Median (Minimum–Maximum Value) | |
|---|---|
| Gestational age at delivery (days) | 258 (207–275) |
| Gestational age at delivery (weeks) | 36.9 (29.6–39.3) |
| Birth weight (g) | 1912 (874–2646) |
| Birth weight (SD) | −2.0 (−3.3 to 1.6) |
| Z score of birth weight | −0.54 (−0.82 to −0.23) |
| Height (cm) | 43 (33.0–48.5) |
| Z score of height | −0.44 (−0.75 to −0.02) |
| Head circumference (cm) | 30.3 (26.5–35.0) |
| Z score of head circumference | −0.27 (−0.69 to 0.36) |
| Estimated fetal weight at the start of treatment (g) | 1130 (309–1714) |
| Z score of estimated fetal weight at the start of treatment | −0.41 (−0.68 to −0.28) |
| Estimated fetal weight at the start of treatment (SD) | −2.1 (−2.8 to −1.5) |
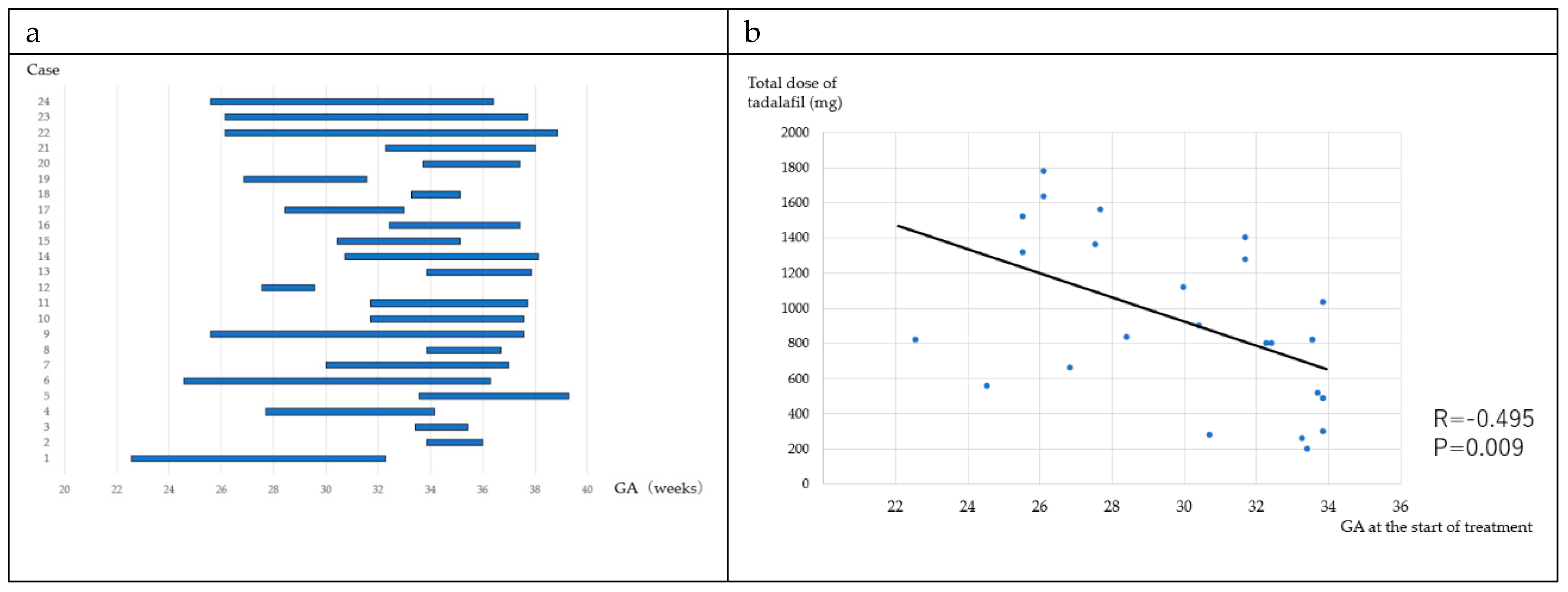
| Gestational age at the start of treatment (days) | 214 (158–237) |
| Gestational age at the start of treatment (weeks) | 30.0 (22.0–33.0) |
| SD: standard deviation |
| 10 mg/day (n = 3) | 20 mg/day (n = 16) | 40 mg/day (n = 5) | Total | |
|---|---|---|---|---|
| BW | ||||
| Catch up + (n) | 2 | 15 | 4 | 21 |
| Catch up − (n) | 1 | 1 | 1 | 3 |
| Catch up (%) | 66.7 | 93.8 | 80.0 | 87.5 |
| Height | ||||
| Catch up + (n) | 2 | 14 | 4 | 20 |
| Catch up − (n) | 1 | 2 | 1 | 4 |
| Catch up (%) | 66.7 | 87.5 | 80.0 | 83.3 |
| Head circumference | ||||
| Catch up + (n) | 3 | 16 | 5 | 24 |
| Catch up − (n) | 0 | 0 | 0 | 0 |
| Catch up (%) | 100 | 100 | 100 | 100 |
| 10 mg/day (n = 3) | 20 mg/day (n = 16) | 40 mg/day (n = 5) | Total | |
|---|---|---|---|---|
| BW (months) | 9 (4–10) | 5.2 (0–12) | 7.3 (4–12) | 5.8 (0–12) |
| Height (months) | 2 (0–4) | 3.8 (0–18) | 5.3 (0–12) | 3.9 (0–18) |
| Head circumference (months) | 6.7 (0–10) | 2.3 (0–10) | 7.2 (0–12) | 3.8 (0–12) |
| DQ | P-M | C-A | L-S | TOTAL n = 18 |
|---|---|---|---|---|
| 10 mg (n = 2) | ||||
| ≦70 | 1 (50.0) | 0 (0) | 0 (0) | 0 (0) |
| 70–85 | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| 85≦ | 1 (50.0) | 2 (100) | 2 (100) | 2 (100) |
| 20 mg (n = 11) | ||||
| ≦70 | 1 (9.0) | 0 (0) | 2 (18.2) | 0 (0) |
| 70–85 | 4 (36.4) | 2 (18.2) | 1 (9.0) | 3 (27.2) |
| 85≦ | 6 (54.5) | 9 (81.8) | 8 (72.7) | 8 (72.7) |
| 40 mg (n = 5) | ||||
| ≦70 | 2 (40.0) | 1 (20.0) | 2 (40.0) | 1 (20.0) |
| 70–85 | 1 (20.0) | 2 (40.0) | 0 (0) | 2 (40.0) |
| 85≦ | 2 (40.0) | 2 (40.0) | 3 (60.0) | 2 (40.0) |
| n = 18 | ||||
|---|---|---|---|---|
| DQ | P-M | C-A | L-S | TOTAL |
| ≦70 | 4 (22.2) | 1 (5.6) | 4 (22.2) | 1 (5.6) |
| 70–85 | 5 (27.8) | 4 (22.2) | 1 (5.6) | 5 (27.7) |
| 85≦ | 9 (50.0) | 13 (72.2) | 13 (72.2) | 12 (61.7) |
| DQ | 10 mg/day (n = 2) | 20 mg/day (n = 11) | 40 mg/day (n = 5) | TOTAL |
|---|---|---|---|---|
| P-M | 81 | 85 | 75 | 82 |
| C-A | 99 | 91 | 85 | 90 |
| L-S | 89 | 91 | 83 | 88 |
| TOTAL | 94 | 88 | 83 | 87 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maki, S.; Kato, I.; Enomoto, N.; Takakura, S.; Nii, M.; Tanaka, K.; Tanaka, H.; Hori, S.; Matsuda, K.; Ueda, Y.; et al. Developmental Evaluation of Infants Who Have Received Tadalafil in Utero for Fetal Growth Restriction. J. Clin. Med. 2020, 9, 1448. https://doi.org/10.3390/jcm9051448
Maki S, Kato I, Enomoto N, Takakura S, Nii M, Tanaka K, Tanaka H, Hori S, Matsuda K, Ueda Y, et al. Developmental Evaluation of Infants Who Have Received Tadalafil in Utero for Fetal Growth Restriction. Journal of Clinical Medicine. 2020; 9(5):1448. https://doi.org/10.3390/jcm9051448
Chicago/Turabian StyleMaki, Shintaro, Ineko Kato, Naosuke Enomoto, Sho Takakura, Masafumi Nii, Kayo Tanaka, Hiroaki Tanaka, Shinsuke Hori, Kana Matsuda, Yukito Ueda, and et al. 2020. "Developmental Evaluation of Infants Who Have Received Tadalafil in Utero for Fetal Growth Restriction" Journal of Clinical Medicine 9, no. 5: 1448. https://doi.org/10.3390/jcm9051448