Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives

 , , , and
, , , and
Abstract
:
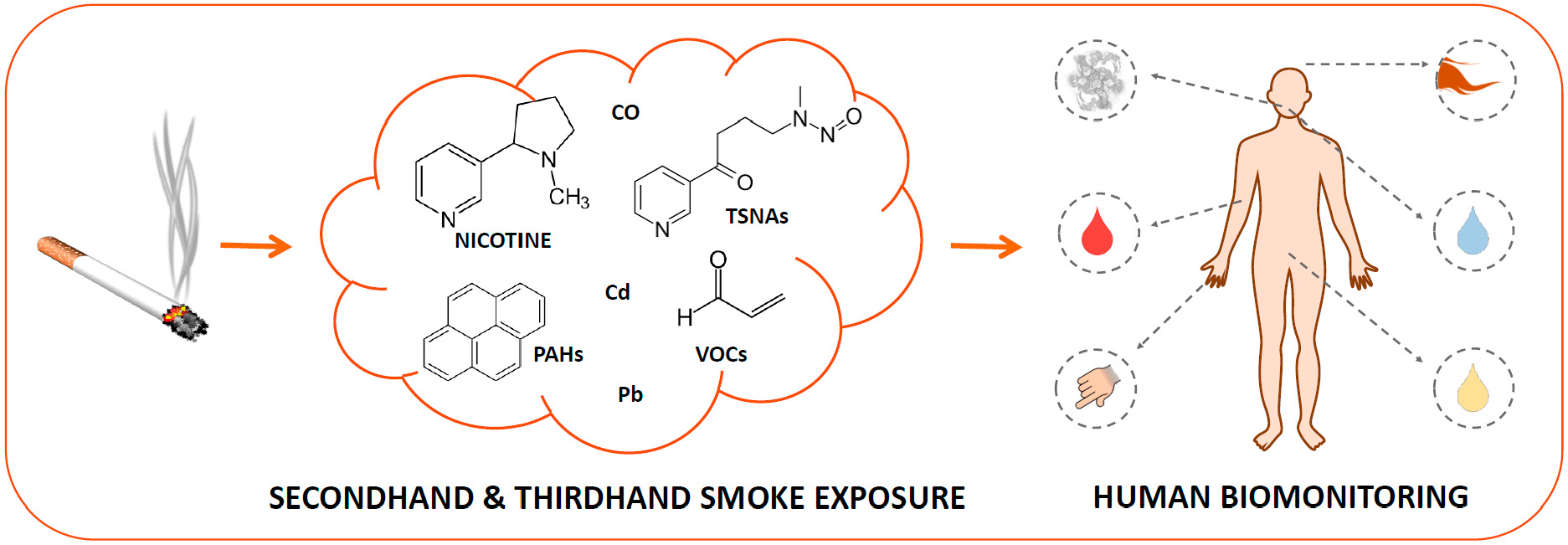
1. Introduction
2. Selection of Papers
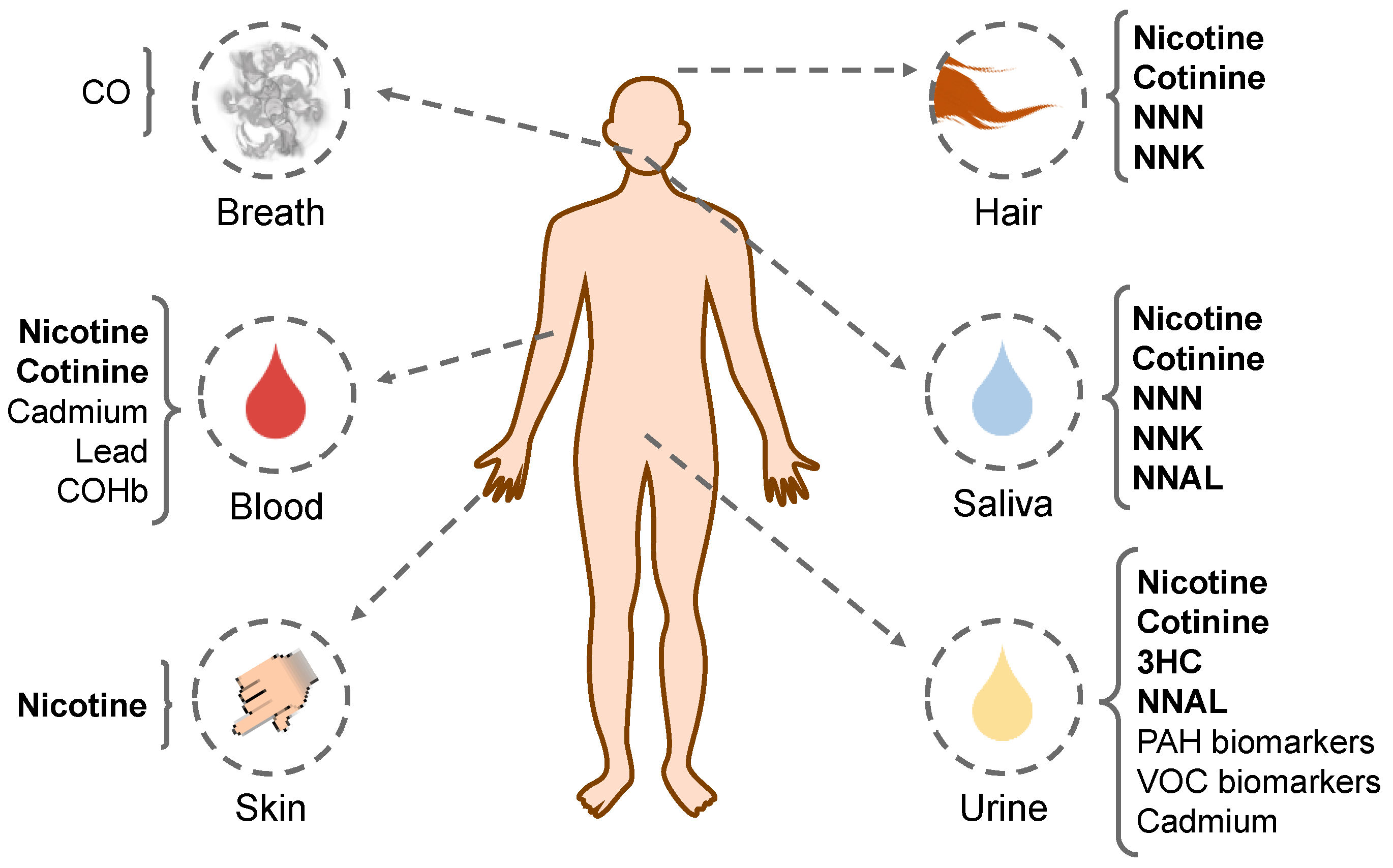
3. Biological Matrices
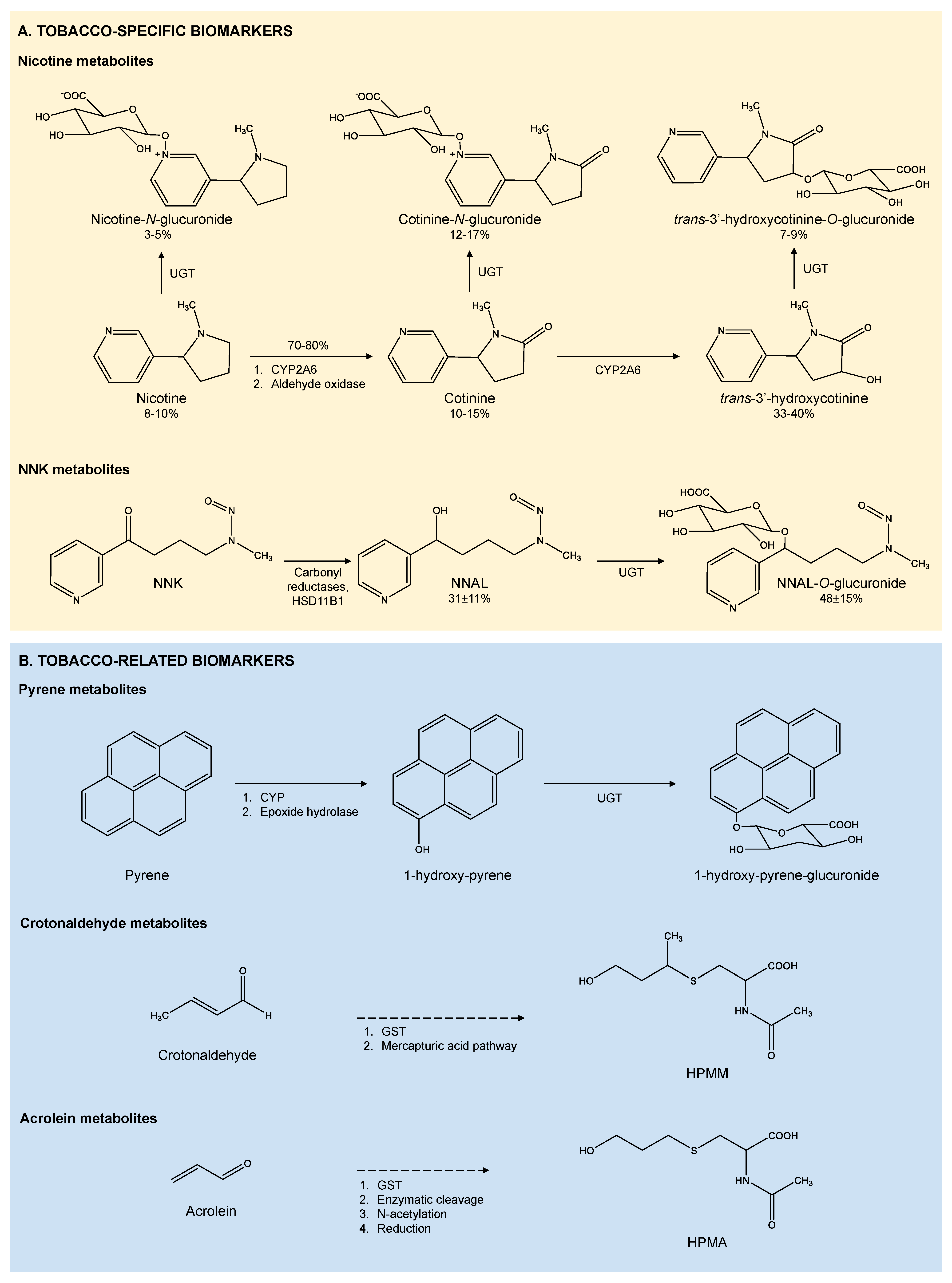
4. Tobacco-Specific Biomarkers
4.1. Nicotine
4.2. Nicotine Metabolites
4.3. Tobacco-Specific Nitrosamines (TSNAs)
5. Tobacco-Related Biomarkers
5.1. Polycyclic Aromatic Hydrocarbons (PAHs)
5.2. Volatile Organic Compounds (VOCs)
5.3. Metals
5.4. Carbon Monoxide
6. Determination of Multiple Specific Biomarkers. Examples of Applications
6.1. Evaluation of SHS Exposure
6.2. Evaluation of THS Exposure
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Pruss-Ustun, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- IARC (International Agency for Reasearch on Cancer). IARC Monographs on Tobacco smoke and involuntary smoking, vol 83. Lyon, France. 2004. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono83.pdf (accessed on 16 May 2018).
- Thielen, A.; Klus, H.; Müller, L. Tobacco smoke: Unraveling a controversial subject. Exp. Toxicol. Pathol. 2008, 60, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Talhout, R.; Schulz, T.; Florek, E.; van Benthem, J.; Wester, P.; Opperhuizen, A. Hazardous compounds in tobacco smoke. Int. J. Environ. Res. Public Health 2011, 8, 613–628. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.E.; Destaillats, H.; Gundel, L.a.; Sleiman, M.; Singer, B.C.; Jacob, P.; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand Tobacco Smoke: Emerging Evidence and Arguments for a Multidisciplinary Research Agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, P.; Benowitz, N.L.; Destaillats, H.; Gundel, L.; Hang, B.; Martins-Green, M.; Matt, G.E.; Quintana, P.J.E.; Samet, J.M.; Schick, S.F.; et al. Thirdhand Smoke: New Evidence, Challenges, and Future Directions. Chem. Res. Toxicol. 2017, 30, 270–294. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, M.; Gundel, L.A.; Pankow, J.F.; Jacob, P.; Singer, B.C.; Destaillats, H. Formation of carcinogens indoors by surface-mediated reactions of nicotine with nitrous acid, leading to potential thirdhand smoke hazards. Proc. Natl. Acad. Sci. USA 2010, 107, 6576–6581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoh, E.; Hunt, R.N.; Quintana, P.J.E.; Zakarian, J.M.; Chatfield, D.A.; Wittry, B.C.; Rodriguez, E.; Matt, G.E. Environmental Tobacco Smoke as a Source of Polycyclic Aromatic Hydrocarbons in Settled Household Dust. Environ. Sci. Technol. 2012, 46, 4174–4183. [Google Scholar] [CrossRef] [PubMed]
- Schick, S.F.; Farraro, K.F.; Perrino, C.; Sleiman, M.; van de Vossenberg, G.; Trinh, M.P.; Katharine Hammond, S.; Jenkins, B.M.; Balmes, J. Thirdhand cigarette smoke in an experimental chamber: Evidence of surface deposition of nicotine, nitrosamines and polycyclic aromatic hydrocarbons and de novo formation of NNK. Tob. Control 2014, 23, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, M.; Logue, J.M.; Luo, W.; Pankow, J.F.; Gundel, L.A.; Destaillats, H. Inhalable Constituents of Thirdhand Tobacco Smoke: Chemical Characterization and Health Impact Considerations. Environ. Sci. Technol. 2014, 48, 13093–13101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez, N.; Özel, M.Z.; Lewis, A.C.; Marcé, R.M.; Borrull, F.; Hamilton, J.F. Exposure to nitrosamines in thirdhand tobacco smoke increases cancer risk in non-smokers. Environ. Int. 2014, 71, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez, N.; Vallecillos, L.; Lewis, A.C.; Borrull, F.; Marcé, R.M.; Hamilton, J.F. Comparative study of comprehensive gas chromatography-nitrogen chemiluminescence detection and gas chromatography-ion trap-tandem mass spectrometry for determining nicotine and carcinogen organic nitrogen compounds in thirdhand tobacco smoke. J. Chromatogr. A 2015, 1426, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Adhami, N.; Starck, S.R.; Flores, C.; Green, M.M. A health threat to bystanders living in the homes of smokers: How smoke toxins deposited on surfaces can cause insulin resistance. PLoS ONE 2016, 11, 1–19. [Google Scholar] [CrossRef]
- Adhami, N.; Chen, Y.; Martins-Green, M. Biomarkers of disease can be detected in mice as early as 4 weeks after initiation of exposure to third-hand smoke levels equivalent to those found in homes of smokers. Clin. Sci. 2017, 131, 2409–2426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins-Green, M.; Adhami, N.; Frankos, M.; Valdez, M.; Goodwin, B.; Lyubovitsky, J.; Dhall, S.; Garcia, M.; Egiebor, I.; Martinez, B.; et al. Cigarette smoke toxins deposited on surfaces: Implications for human health. PLoS ONE 2014, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hang, B.; Sarker, A.H.; Havel, C.; Saha, S.; Hazra, T.K.; Schick, S.; Jacob, P.; Rehan, V.K.; Chenna, A.; Sharan, D.; et al. Thirdhand smoke causes DNA damage in human cells. Mutagenesis 2013, 28, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Avila-Tang, E.; Al-Delaimy, W.K.; Ashley, D.L.; Benowitz, N.; Bernert, J.T.; Kim, S.; Samet, J.M.; Hecht, S.S. Assessing secondhand smoke using biological markers. Tob. Control 2013, 22, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.I.; Dains, K.M.; Dempsey, D.; Herrera, B.; Yu, L.; Jacob, P. Urine nicotine metabolite concentrations in relation to plasma cotinine during low-level nicotine exposure. Nicotine Tob. Res. 2009, 11, 954–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wassenaar, C.A.; Conti, D.V.; Das, S.; Chen, P.; Cook, E.H.; Ratain, M.J.; Benowitz, N.L.; Tyndale, R.F. UGT1A and UGT2B Genetic Variation Alters Nicotine and Nitrosamine Glucuronidation in European and African American Smokers. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Schultze, B.; Lind, P.M.; Larsson, A.; Lind, L. Whole blood and serum concentrations of metals in a Swedish population-based sample. Scand. J. Clin. Lab. Invest. 2014, 74, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Pearl, M.; Jacob, P.; DeLorenze, G.N.; Benowitz, N.L.; Yu, L.; Havel, C.; Kharrazi, M. Levels of cotinine in dried blood specimens from newborns as a biomarker of maternal smoking close to the time of delivery. Am. J. Epidemiol. 2013, 178, 1648–1654. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Hanke, W.; Sobala, W.; Trzcinka-Ochocka, M.; Ligocka, D.; Brzeznicki, S.; Strugala-Stawik, H.; Magnus, P. Developmental Effects of Exposures to Environmental Factors: The Polish Mother and Child Cohort Study. Biomed Res. Int. 2013, 2013, 629716. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ortuño, R.; Martínez-Sánchez, J.M.; Fu, M.; Fernández, E.; Pascual, J.A. Evaluation of tobacco specific nitrosamines exposure by quantification of 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) in human hair of non-smokers. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P. Nicotine chemistry, Metabolism, Kinetics and Biomarkers. Handb. Exp. Pharmacol. 2009, 192, 29–60. [Google Scholar] [CrossRef]
- Al-Delaimy, W.K. Hair as a biomarker for exposure to tobacco smoke. Tob. Control 2002, 11, 176–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. EPA (U.S. Environmental Protection Agency). Dermal exposure assessment: A summary of epa approaches. U.S. Environmental Protection Agency, Washington, DC, EPA/600/R-07/040F. 2007. Available online: https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=183584 (accessed on 2 July 2018).
- Weschler, C.J.; Nazaroff, W.W. Dermal Uptake of Organic Vapors Commonly Found in Indoor Air. Environ. Sci. Technol. 2014, 48, 1230–1237. [Google Scholar] [CrossRef] [PubMed]
- Deveci, S.E.; Deveci, F.; Açik, Y.; Ozan, A.T. The measurement of exhaled carbon monoxide in healthy smokers and non-smokers. Respir. Med. 2004, 98, 551–556. [Google Scholar] [CrossRef] [PubMed]
- OEHHA-CalEPA Chemical Database CalEPA. Toxicity Criteria on Chemicals Evaluated by OEHHA. California Environmental Protection Agency. 2018. Available online: https://oehha.ca.gov/chemicals (accessed on 4 June 2018).
- IARC (International Agency for Research on Cancer). List of classifications by alphabetical order. 2013. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/07/ClassificationsAlphaOrder.pdf (accessed on 15 May 2018).
- Naufal, Z.; Kathman, S.; Wilson, C. Bayesian derivation of an oral cancer slope factor distribution for 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK). Regul. Toxicol. Pharmacol. 2009, 55, 69–75. [Google Scholar] [CrossRef] [PubMed]
- RAIS: RAIS (The Risk Assessment Information System); 2009. Available online: https://rais.ornl.gov/tools/tox_profiles.html (accessed on 7 June 2018).
- OEHHA-CalEPA. Air Toxics Hot Spots Program Risk Assessment Guidelines. Part I: The Determination of Acute Reference Exposure Levels for Airborne Toxicants. 1999. Available online: https://oehha.ca.gov/media/downloads/crnr/acuterel.pdf (accessed on 11 June 2018).
- EPA (United States Environmental Protection Agency). Basic Information about the Integrated Risk Information System. Available online: https://www.epa.gov/iris/basic-information-about-integrated-risk-information-system (accessed on 3 June 2018).
- Tzatzarakis, M.N.; Vardavas, C.I.; Terzi, I.; Kavalakis, M.; Kokkinakis, M.; Liesivuori, J.; Tsatsakis, A.M. Hair nicotine/cotinine concentrations as a method of monitoring exposure to tobacco smoke among infants and adults. Hum. Exp. Toxicol. 2012, 31, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Moon, K.A.; Rule, A.M.; Magid, H.S.; Ferguson, J.M.; Susan, J.; Sun, Z.; Torrey, C.; Abubaker, S.; Levshin, V.; Çarkoglu, A.; et al. Biomarkers of secondhand smoke exposure in waterpipe tobacco venue employees in Istanbul, Moscow, and Cairo. Nicotine Tob. Res. 2018, 20, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Park, E.Y.; Yun, E.H.; Lim, M.K.; Lee, D.-H.; Yang, W.; Jeong, B.Y.; Hwang, S.-H. Consequences of incomplete smoke-free legislation in the Republic of Korea: Results from environmental and biochemical monitoring: Community based study. Cancer Res. Treat. 2016, 48, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Apelberg, B.J.; Avila-Tang, E.; Hepp, L.; Yun, D.; Samet, J.M.; Breysse, P.N. Utility and Cutoff Value of Hair Nicotine as a Biomarker of Long-Term Tobacco Smoke Exposure, Compared to Salivary Cotinine. Int. J. Environ. Res. Public Health 2014, 11, 8368–8382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoli, C. A Comparison of Survey Measures and Biomarkers of Secondhand Tobacco Smoke Exposure among Nonsmokers. Public Health Nurs. 2016, 33, 82–89. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.J.; Racicot, S.; Okoli, C.T.C.; Hammond, S.K.; O’Loughlin, J. Airborne Nicotine, Secondhand Smoke, and Precursors to Adolescent Smoking. Pediatrics 2018, 141, S63–S74. [Google Scholar] [CrossRef] [PubMed]
- Northrup, T.F.; Khan, A.M.; Jacob, P.; Benowitz, N.L.; Hoh, E.; Hovell, M.F.; Matt, G.E.; Stotts, A.L. Thirdhand smoke contamination in hospital settings: Assessing exposure risk for vulnerable paediatric patients. Tob. Control 2016, 25, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.E.; Zakarian, J.M.; Hoh, E.; Hovell, M.F.; Mahabee-Gittens, M.; Watanabe, K.; Datuin, K.; Vue, C.; Chatfield, D.A. When smokers quit: Exposure to nicotine and carcinogens persists from thirdhand smoke pollution. Tob. Control 2017, 26, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.E.; Fortmann, A.L.; Zakarian, J.M.; Galaviz, V.E.; Chatfield, D.A.; Hoh, E.; Hovell, M.F.; Winston, C. Thirdhand smoke and exposure in California hotels: Non-smoking rooms fail to protect non-smoking hotel guests from tobacco smoke exposure. Tob. Control 2014, 23, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.; Shamo, F.; Boynton, K.; Kiley, J. The impact of Michigan’s Dr Ron Davis smoke-free air law on levels of cotinine, tobacco-specific lung carcinogen and severity of self-reported respiratory symptoms among non-smoking bar employees. Tob. Control 2012, 21, 593–595. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, A.; Matsumoto, A.; Ichiba, M.; Payton, N.M.; Oishi, H.; Hara, M. Simultaneous measurement of urinary total nicotine and cotinine as biomarkers of active and passive smoking among Japanese individuals. Environ. Health Prev. Med. 2013, 18, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Forysová, K.; Pinkr-Grafnetterová, A.; Malý, M.; Krsková, A.; Mráz, J.; Kašparová, L.; Čejchanová, M.; Sochorová, L.; Rödlová, S.; Černá, M. Urinary Cadmium and Cotinine Levels and Hair Mercury Levels in Czech Children and Their Mothers Within the Framework of the COPHES/DEMOCOPHES Projects. Arch. Environ. Contam. Toxicol. 2017, 73, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Caman, O.K.; Erguder, B.I.; Ozcebe, H.; Bilir, N. Urinary Cotinine and Breath Carbon Monoxide Levels Among Bar and Restaurant Employees in Ankara. Nicotine Tob. Res. 2013, 15, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Fthenou, E.; Patelarou, E.; Bagkeris, E.; Murphy, S.; Hecht, S.S.; Connolly, G.N.; Chatzi, L.; Kogevinas, M. Exposure to different sources of secondhand smoke during pregnancy and its effect on urinary cotinine and tobacco-specific nitrosamine (NNAL) concentrations. Tob. Control 2013, 22, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.A.; St Helen, G.; Meyers, M.J.; Dempsey, D.A.; Havel, C.; Jacob, P.; Northcross, A.; Hammond, S.K.; Benowitz, N.L. Biomarkers of secondhand smoke exposure in automobiles. Tob. Control 2014, 23, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Nardone, N.; Jain, S.; Dempsey, D.A.; Addo, N.; St. Helen,, G.; Jacob, P. Comparison of Urine 4-(Methylnitrosamino)-1-(3)Pyridyl-1-Butanol and Cotinine for Assessment of Active and Passive Smoke Exposure in Urban Adolescents. Cancer Epidemiol. Biomarkers Prev. 2018, 27, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Ho, G.; Tang, H.; Robbins, J.A.; Tong, E.K. Biomarkers of Tobacco Smoke Exposure and Asthma Severity in Adults. Am. J. Prev. Med. 2013, 45, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.E.; Wickham, K.M.; Lindgren, B.R.; Spector, L.G.; Joseph, A. Cotinine and trans 3′-hydroxycotinine in dried blood spots as biomarkers of tobacco exposure and nicotine metabolism. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 513–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, B.F.; Clark, M.L.; Bachand, A.; Reynolds, S.J.; Nelson, T.L.; Peel, J.L. Interactions Between Diet and Exposure to Secondhand Smoke on Metabolic Syndrome Among Children: NHANES 2007-2010. J. Clin. Endocrinol. MeTable 2016, 101, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Wei, B.; Blount, B.C.; Xia, B.; Wang, L. Assessing exposure to tobacco-specific carcinogen NNK using its urinary metabolite NNAL measured in US population: 2011–2012. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Bagchi, P.; Geldner, N.; DeCastro, B.R.; De Jesús, V.R.; Park, S.K.; Blount, B.C. Crotonaldehyde exposure in U.S. tobacco smokers and nonsmokers: NHANES 2005–2006 and 2011–2012. Environ. Res. 2018, 163, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.A.; Perera, F.P.; Maugeri, U.; Spengler, J.; Mroz, E.; Flak, E.; Stigter, L.; Majewska, R.; Kaim, I.; Sowa, A.; et al. Prohypertensive Effect of Gestational Personal Exposure to Fine Particulate Matter. Prospective Cohort Study in Non-smoking and Non-obese Pregnant Women. Cardiovasc. Toxicol. 2012, 12, 216–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-W.; Kam, S.; Lee, D.-H. Synergistic interaction between polycyclic aromatic hydrocarbons and environmental tobacco smoke on the risk of obesity in children and adolescents: The U.S. National Health and Nutrition Examination Survey 2003–2008. Environ. Res. 2014, 135, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.B. Serum cotinine and urinary 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanonol levels among non-Hispanic Asian American smokers and nonsmokers as compared to other race/ethnicities: Data from NHANES 2011–2012. Chemosphere 2015, 120, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.; Kvaavik, E.; Hamer, M.; Batty, G.D. Association of secondhand smoke exposure with mental health in men and women: Cross-sectional and prospective analyses using the UK Health and Lifestyle Survey. Eur. Psychiatry 2013, 28, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ortuño, R.; Martínez-Sánchez, J.M.; Fu, M.; Ballbè, M.; Quirós, N.; Fernández, E.; Pascual, J.A. Assessment of tobacco specific nitrosamines (TSNAs) in oral fluid as biomarkers of cancer risk: A population-based study. Environ. Res. 2016, 151, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Helen, G.; Thomas Bernert, J.; Hall, D.B.; Sosnoff, C.S.; Xia, Y.; Balmes, J.R.; Vena, J.E.; Wang, J.-S.; Holland, N.T.; Naeher, L.P. Exposure to Secondhand Smoke Outside of a Bar and a Restaurant and Tobacco Exposure Biomarkers in Nonsmokers. Environ. Health Perspect. 2012, 120, 1010–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, S.; Huynh, C.K.; Bauer, G.F.; Hoffmann, S.; Röösli, M. Impact of a smoking ban in hospitality venues on second hand smoke exposure: A comparison of exposure assessment methods. BMC Public Health 2013, 13, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Matt, G.E. Preliminary evidence that high levels of nicotine on children’s hands may contribute to overall tobacco smoke exposure. Tob. Control 2018, 27, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, M.; Kanda, H.; Hayakawa, T.; Mori, Y.; Ito, T.; Hidaka, T.; Kakamu, T.; Kumagai, T.; Osaki, Y.; Kawazoe, M.; et al. Nicotine cut-off value in human hair as a tool to distinguish active from passive smokers: A cross-sectional study in Japanese men. Cancer Biomarkers 2017, 20, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Szumska, M.; Tyrpień, K.; Kowalska, M.; Wielkoszyński, T.; Dobosz, C. Medicine students and exposure to environmental tobacco smoke. Int. J. Occup. Med. Environ. Health 2013, 26, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schick, S.F.; Van Den Vossenberg, G.; Luo, A.; Whitlatch, A.; Jacob, P.; Balmes, J.; Shusterman, D. Thirty minute-exposure to aged cigarette smoke increases nasal congestion in nonsmokers. J. Toxicol. Environ. Health Part A Curr. Issues 2013, 76, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Protano, C.; Andreoli, R.; Manini, P.; Guidotti, M.; Vitali, M. A tobacco-related carcinogen: Assessing the impact of smoking behaviours of cohabitants on benzene exposure in children. Tob. Control 2012, 21, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Kassem, N.O.F.; Kassem, N.O.; Liles, S.; Zarth, A.T.; Jackson, S.R.; Daffa, R.M.; Chatfield, D.A.; Carmella, S.G.; Hecht, S.S.; Hovell, M.F. Acrolein Exposure in Hookah Smokers and Non-Smokers Exposed to Hookah Tobacco Secondhand Smoke: Implications for Regulating Hookah Tobacco Products. Nicotine Tob. Res. 2018, 20, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Lee, S.; Roh, J.; Won, J.U.; Yoon, J.H. The Association between Involuntary Smoking Exposure with Urine Cotinine Level and Blood Cadmium Level in General Non-Smoking Populations. J. Korean Med. Sci. 2017, 32, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Bentur, L.; Hellou, E.; Goldbart, A.; Pillar, G.; Monovich, E.; Salameh, M.; Scherb, I.; Bentur, Y. Laboratory and Clinical Acute Effects of Active and Passive Indoor Group Water-Pipe (Narghile) Smoking. Chest 2014, 145, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Catassi, A.; Servent, D.; Paleari, L.; Cesario, A.; Russo, P. Multiple roles of nicotine on cell proliferation and inhibition of apoptosis: Implications on lung carcinogenesis. Mutat. Res. - Rev. Mutat. Res. 2008, 659, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L. Nicotine Addiction. N Engl J Med 2010, 362, 2295–2303. [Google Scholar] [CrossRef] [PubMed]
- Hukkanen, J.; Jacob, P.; Benowitz, N.L.; Jacob, P. Metabolism and Disposition Kinetics of Nicotine. Pharmacol. Rev. 2005, 57, 79–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uematsu, T.; Mizuno, A.; Nagashima, S.; Oshima, A.; Nakamura, M. The axial distribution of nicotine content along hair shaft as an indicator of changes in smoking behaviour: Evaluation in a smoking- cessation programme with or without the aid of nicotine chewing gum. Br. J. Clin. Pharmacol. 1995, 39, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Jacob, P. Metabolism of nicotine to cotinine studied by a dual stable isotope method. Clin. Pharmacol. Ther. 1994, 56, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Murphy, P.J. Enzymatic oxidation of nicotine to nicotine 1’(5’) iminium ion. A newly discovered intermediate in the metabolism of nicotine. J. Biol. Chem. 1973, 248, 2796–2800. [Google Scholar] [PubMed]
- Brandänge, S.; Lindblom, L. The enzyme “aldehyde oxidase” is an iminium oxidase. Reaction with nicotine Δ1′(5′) iminium ion. Biochem. Biophys. Res. Commun. 1979, 91, 991–996. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Jacob, P. Nicotine and cotinine elimination pharmacokinetics in smokers and nonsmokers. Clin. Pharmacol. Ther. 1993, 53, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.E.; Johnson, L.M.; Pullo, D.A. Characterization of multiple products of cytochrome P450 2A6-catalyzed cotinine metabolism. Chem. Res. Toxicol. 1999, 12, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Jacob, P. Trans-3′-hydroxycotinine: Disposition kinetics, effects and plasma levels during cigarette smoking. Br. J. Clin. Pharmacol. 2008, 51, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Hagan, R.L.; Ramos, J.M.; Jacob, P.M. Increasing urinary cotinine concentrations at elevated temperatures: The role of conjugated metabolites. J. Pharm. Biomed. Anal. 1997, 16, 191–197. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Kuyt, F.; Jacob, P.; Jones, R.T.; Osman, A.-L. Cotinine disposition and effects. Clin. Pharmacol. Ther. 1983, 34, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Jacob, P.; Fong, I.; Gupta, S. Nicotine metabolic profile in man: Comparison of cigarette smoking and transdermal nicotine. J. Pharmacol. Exp. Ther. 1994, 268, 296–303. [Google Scholar] [PubMed]
- Hecht, S.S.; Stepanov, I.; Carmella, S.G. Exposure and Metabolic Activation Biomarkers of Carcinogenic Tobacco-Specific Nitrosamines. Acc. Chem. Res. 2016, 49, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Luukkanen, L.; Mikkola, J.; Forsman, T.; Taavitsainen, P.; Taskinen, J.; Elovaara, E. Glucuronidation of 1-Hydroxypyrene by Human Liver Microsomes and Human UDP-Glucuronosyltransferases UGT1A6, UGT1A7, and UGT1A9: Development of a High-Sensitivity Glucuronidation Assay for Human Tissue. Drug Metab. Dispos. 2001, 29, 1096–1101. [Google Scholar] [PubMed]
- CDC (Centers for Disease Control). Urinary Volatile Organic Compound Metabolites: Reference Ranges, Chemical Structures and Parent Compounds Volatile Organic Compounds Laboratory, CDC/DLS/Tobacco and Volatiles Branch. 2017. Available online: https://biomonitoring.ca.gov/sites/default/files/downloads/CDC_VOCMetaboliteTable_July2017.pdf (accessed on 18 June 2018).
- Stevens, J.F.; Maier, C.S. Acrolein: Sources, metabolism, and biomolecular interactions relevant to human health and disease. Mol. Nutr. Food Res. 2008, 52, 7–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC (International Agency for Research on Cancer). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Smokeless Tobacco and Some Tobacco-specific Nitrosamines, vol. 89. Lyon, France: WHO. 2007. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono89.pdf (accessed on 30 May 2018).
- Hecht, S.S. Tobacco Smoke Carcinogens and Lung Cancer. J. Natl. Cancer Inst. 1999, 91, 1194–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, D.; Hecht, S.S. Nicotine-derived N-Nitrosamines and Tobacco-related Cancer: Current Status and Future Directions. Cancer Res. 1985, 45, 935–944. [Google Scholar] [PubMed]
- Hecht, S.S. Biochemistry, Biology, and Carcinogenicity of Tobacco-Specific N-Nitrosamines. Chem. Res. Toxicol. 1998, 11, 559–603. [Google Scholar] [CrossRef] [PubMed]
- Breyer-Pfaff, U.; Martin, H.-J.; Ernst, M.; Maser, E. Enantioselectivity of carbonyl reduction of 4-methylnitrosamino-1-(3-pyridyl)-1-butanone by tissue fractions from human and rat and by enzymes isolated from human liver. Drug Metab. Dispos. 2004, 32, 915–922. [Google Scholar] [PubMed]
- Yuan, J.-M.; Koh, W.-P.; Murphy, S.E.; Fan, Y.; Wang, R.; Carmella, S.G.; Han, S.; Wickham, K.; Gao, Y.-T.; Yu, M.C.; et al. Urinary levels of tobacco-specific nitrosamine metabolites in relation to lung cancer development in two prospective cohorts of cigarette smokers. Cancer Res. 2009, 69, 2990–2995. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.-M.; Knezevich, A.D.; Wang, R.; Gao, Y.-T.; Hecht, S.S.; Stepanov, I. Urinary levels of the tobacco-specific carcinogen N’-nitrosonornicotine and its glucuronide are strongly associated with esophageal cancer risk in smokers. Carcinogenesis 2011, 32, 1366–1371. [Google Scholar] [CrossRef] [PubMed]
- Carmella, S.G.; Ming, X.; Olvera, N.; Brookmeyer, C.; Yoder, A.; Hecht, S.S. High throughput liquid and gas chromatography-tandem mass spectrometry assays for tobacco-specific nitrosamine and polycyclic aromatic hydrocarbon metabolites associated with lung cancer in smokers. Chem. Res. Toxicol. 2013, 26, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.; Slezakova, K.; Delerue-Matos, C.; da Conceição Alvim-Ferraz, M.; Morais, S.; do Carmo Pereira, M. Polycyclic aromatic hydrocarbons in gas and particulate phases of indoor environments influenced by tobacco smoke: Levels, phase distributions, and health risks. Atmos. Environ. 2011, 45, 1799–1808. [Google Scholar] [CrossRef] [Green Version]
- Ewa, B.; Danuta, M.-Š. Polycyclic aromatic hydrocarbons and PAH-related DNA adducts. J. Appl. Genet. 2017, 58, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Gil, L.; Adonis, M. Genomics and proteomics offers new hopes towards a personalized approach to lung cancer prevention and treatment. Electron. J. Biotechnol. 2003, 6. [Google Scholar] [CrossRef]
- St Helen, G.; Goniewicz, M.L.; Dempsey, D.; Wilson, M.; Jacob, P.; Benowitz, N.L. Exposure and Kinetics of Polycyclic Aromatic Hydrocarbons (PAHs) in Cigarette Smokers. Chem. Res. Toxicol. 2012, 25, 952–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). Air Quality Guidelines for Europe. Second Edition. 2000. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/74732/E71922.pdf (accessed on 15 July 2018).
- Kim, K.-H.; Jahan, S.A.; Kabir, E.; Brown, R.J.C. A review of airborne polycyclic aromatic hydrocarbons (PAHs) and their human health effects. Environ. Int. 2013, 60, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Wilson, V.L.; Foiles, P.G.; Chung, F.-L.; Povey, A.C.; Frank, A.A.; Harris, C.C. Detection of acrolein and crotonaldehyde DNA adducts in cultured human cells and canine peripheral blood lymphocytes by 32P-postlabeling and nucleotide chromatography. Carcinogenesis 1991, 12, 1483–1490. [Google Scholar] [CrossRef] [PubMed]
- Snyder, R.; Hedli, C.C. An overview of benzene metabolism. Environ. Health Perspect. 1996, 104, 1165–1171. [Google Scholar] [PubMed]
- Snyder, R. Leukemia and benzene. Int. J. Environ. Res. Public Health 2012, 9, 2875–2893. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.O.; Minet, E.; McEwan, M. Urinary biomarkers of smokers’ exposure to tobacco smoke constituents in tobacco products assessment: A fit for purpose approach. Biomarkers 2013, 18, 467–486. [Google Scholar] [CrossRef] [PubMed]
- Waidyanatha, S.; Rothman, N.; Fustinoni, S.; Smith, M.T.; Hayes, R.B.; Bechtold, W.; Dosemeci, M.; Guilan, L.; Yin, S.; Rappaport, S.M. Urinary benzene as a biomarker of exposure among occupationally exposed and unexposed subjects. Carcinogenesis 2001, 22, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreoli, R.; Spatari, G.; Pigini, D.; Poli, D.; Banda, I.; Goldoni, M.; Riccelli, M.G.; Petyx, M.; Protano, C.; Vitali, M.; Barbaro, M.; Mutti, A. Urinary biomarkers of exposure and of oxidative damage in children exposed to low airborne concentrations of benzene. Environ. Res. 2015, 142, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, D.; Rossmann, A.; Wick, G. Metals in cigarette smoke. IUBMB Life (Int. Union Biochem. Mol. Biol. Life) 2005, 57, 805–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Järup, L. Hazards of heavy metal contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabinowitz, M.B.; Wetherill, G.W.; Kopple, J.D. Kinetic analysis of lead metabolism in healthy humans. J. Clin. Invest. 1976, 58, 260–270. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization) Task Group on Environmental Health Criteria for Cadmium; Friberg, L.; Elinder, C.-G.; Kjellström, T.; United Nations Environment Programme; International Labour Organisation; World Health Organization. International Program on Chemical Safety. Cadmium. Geneva, Switzerland. 1992. Available online: http://www.inchem.org/documents/ehc/ehc/ehc134.htm (accessed on 3 July 2018).
- Richter, P.; Faroon, O.; Pappas, R.S. Cadmium and Cadmium/Zinc Ratios and Tobacco-Related Morbidities. Int. J. Environ. Res. Public Health 2017, 14, 1154. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Ujjin, P.; Vanavanitkun, Y.; Nishijo, M.; Baker, J.R.; Moore, M.R. Effects of cigarette smoking and exposure to cadmium and lead on phenotypic variability of hepatic CYP2A6 and renal function biomarkers in men. Toxicology 2004, 204, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.; Spector, L.; Wickham, K.; Janis, G.; Winickoff, J.; Lindgren, B.; Murphy, S. Biomarker evidence of tobacco smoke exposure in children participating in lead screening. Am. J. Public Health 2013, 103, e54–e59. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.F.; Chan, I.H.S.; Liu, T.C.; Lam, C.W.K.; Wong, G.W.K. Relationship Between Passive Smoking Exposure and Urinary Heavy Metals and Lung Functions in Preschool Children. Pediatr. Pulmonol. 2013, 48, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, J.E.; Bartolomé, M.; Cañas, A.I.; Huetos, O.; Navarro, C.; Rodríguez, A.C.; Arribas, M.; Esteban, M.; López, A.; Castaño, A. Anti-smoking legislation and its effects on urinary cotinine and cadmium levels. Environ. Res. 2015, 136, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Czogala, J.; Goniewicz, M.L. The Complex Analytical Method for Assessment of Passive Smokers’ Exposure to Carbon Monoxide. J. Anal. Toxicol. 2005, 29, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Raub, J.A.; Mathieu-Nolf, M.; Hampson, N.B.; Thom, S.R. Carbon monoxide poisoning—A public health perspective. Toxicology 2000, 145, 1–14. [Google Scholar] [CrossRef]
- Czogala, J.; Goniewicz, M.L. Carbon monoxide levels in main- and sidestream smoke from cigarettes of selected brands and estimation of active and passive smokers exposure to this compound. Ann Pol Chem Soc. 2003, 2, 316–320. [Google Scholar]
- Secker-Walker, R.; Vacek, P.; Flynn, B.; Mead, P. Smoking in Pregnancy, Exhaled Carbon Monoxide, and Birth Weight. Obstet. Gynecol. 1997, 89, 648–653. [Google Scholar] [CrossRef]
- Zhou, S.; Behrooz, L.; Weitzman, M.; Pan, G.; Vilcassim, R.; Mirowsky, J.E.; Breysee, P.; Rule, A.; Gordon, T. Secondhand hookah smoke: An occupational hazard for hookah bar employees. Tob. Control 2017, 26, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, K.; Kwon, H.-J.; Lee, D.H.; Kim, K. Association between Secondhand Smoke in Hospitality Venues and Urinary 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol Concentrations in Non-Smoking Staff. Int. J. Environ. Res. Public Health 2016, 13, 1101. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kwon, H.-J.; Lee, K.; Lee, D.-H.; Paek, Y.; Kim, S.-S.; Hong, S.; Lim, W.; Heo, J.-H.; Kim, K. Air Quality, Biomarker Levels, and Health Effects on Staff in Korean Restaurants and Pubs Before and After a Smoking Ban. Nicotine Tob. Res. 2015, 17, 1337–1346. [Google Scholar] [CrossRef] [PubMed]
- Bekö, G.; Morrison, G.; Weschler, C.; Koch, H.; Palmke, C.; Salthammer, T.; Schripp, T.; Toftum, J.; Clausen, G. Measurements of dermal update of nicotine directly from air and clothing. Indoor Air 2017, 27, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Bekö, G.; Morrison, G.; Weschler, C.J.; Koch, H.M.; Pälmke, C.; Salthammer, T.; Schripp, T.; Eftekhari, A.; Toftum, J.; Clausen, G. Dermal uptake of nicotine from air and clothing: Experimental verification. Indoor Air 2018, 28, 247–257. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Biomarker | Half-Life Time (t1/2) a | Toxicant Precursor | IARC Classification b | Cancer | Non-Cancer | Other | |
|---|---|---|---|---|---|---|---|
| Inhalation Unit Risk | Slope Factor | Chronic Inhalation REL | |||||
| Tobacco smoke specific biomarkers | |||||||
| Nicotine | Blood (t1/2): 2 h Urine (t1/2): 11 h | Nicotine | NA | NA | NA | NA | Reproductive toxicity |
| Cotinine | Saliva (t1/2): 15 h Blood (t1/2): 16 h Urine (t1/2): 3–4 days | ||||||
| trans-3’-hydroxycotinine (3HC) | Blood (t1/2): 6.6 h Urine (t1/2): 6.4 h | ||||||
| N′-nitrosonornicotine (NNN) | NA | NNN | 1 | 4.0 × 10−4 | 1.4 | NA | NSRL: 0.5 µg/day |
| 4-(methylnitrosoamino)-1-(3-pyridyl)-1-butanone (NNK) | Urine (t1/2): 2.6 h | NNK | 1 | 5.2 × 10−3 c | 49 (oral) | NA | NSRL: 0.014 µg/day |
| 4-(methylnitrosoamino)-1-(3-pyridyl)-1-butanol (NNAL) | Urine (t1/2): 40–45 days | ||||||
| Tobacco smoke related biomarkers | |||||||
| Polycyclic aromatic hydrocarbon biomarkers | |||||||
| 1-hydroxy naphthalene (1-OHNap) 2-hydroxy naphthalene (2-OHNap) | NA | Naphthalene | 2B | 3.4 × 10−5 | 0.12 | 9 | NSRL: 5.8 µg/day |
| Urine (t1/2): 9.4 h | |||||||
| 2-hydroxy fluorene (2-OHFlu) 3-hydroxy fluorene (3-OHFlu) 9-hydroxy fluorene (9-OHFlu) | Urine (t1/2): 4.1 h | Fluorene | 3 | NA | NA | NA | NA |
| NA | |||||||
| NA | |||||||
| 1-hydroxy phenanthrene (1-OHPA) 2-hydroxy phenanthrene (2-OHPA) 3-hydroxy phenanthrene (3-OHPA) | NA | Phenanthrene | 3 | NA | NA | NA | NA |
| NA | |||||||
| NA | |||||||
| 1-hydroxy-pyrene (1-OHPyr) 1-hydroxy-pyrene glucuronide (1-OHPyrG) | Urine (t1/2): 6 h NA | Pyrene | 3 | NA | NA | NA | NA |
| Volatile organic compounds biomarkers | |||||||
| Benzene | NA | Benzene | 1 | 2.9 × 10−5 | 0.1 | 3 | Reproductive toxicity NSRL: 13 (inhalation) 6.4 (oral) µg/day |
| N-acetyl-S-(3-hydroxypropyl-1-methyl)-L-cysteine (HPMM) | Urine (t1/2): 5–9 h | Crotonaldehyde | 3 | NA | 1.9 (oral) d | NA | NA |
| 3-hydroxypropyl mercapturic acid (HPMA) | Urine (t1/2): 5–9 h | Acrolein | 3 | NA | NA | 0.35 | NA |
| Metals | |||||||
| Cadmium | Blood and urine (t1/2): 1–2 decades | Cadmium | 1 | 4.2 × 10−3 | 15 | 0.02 | Reproductive toxicity NSRL (inhalation): 0.05 µg/day |
| Lead | Blood (t1/2): 36 days | Lead | 2B | 1.2 × 10−5 | 0.042 (inhalation) 8.5 × 10−3 (oral) | NA | Reproductive toxicity NSRL (oral): 15 µg/day |
| Other | |||||||
| Carbon monoxide (CO) Carboxyhemoglobin (COHb) | Exhaled (t1/2): 2–6 h | CO | NA | NA | NA | 23,000 (acute REL) | Reproductive toxicity |
| Blood (t1/2): 4–6 h | |||||||
| Biomarker | Matrix | Smokers | SHS Exposure | THS Exposure | No Exposure | References |
|---|---|---|---|---|---|---|
| Nicotine | Hair | 2.01–79.30 ng/mg (min–max) | 0.08–5.02 ng/mg (IQR) | NA | NA | [23,35,36,37,38,39,40] |
| Skin | 44–1160 ng/wipe (min–max) | 25.6 (13.2–48.9) ng/wipe (GM (95% CI)) | 2.9 (<LOD–46.1) ng/wipe (GM (95% CI) | 2.5 (<LOD–17.7) ng/wipe (GM (min–max)) | [41,42,43] | |
| Cotinine | Urine | 34.5–489.15 ng/mL (GM range) | 0.25–30 ng/mL (min–cutoff point) | 0.05–5 ng/mL (Cutoff range) | 0.88 ng/mL (max value) | [22,36,41,42,43,44,45,46,47,48,49,50] |
| Serum/Plasma | >10–499 ng/mL (cutoff–max) | 0.015–14.6 ng/mL (Cutoff range) | NA | <LOD (<0.05) ng/mL | [49,51,52,53,54,55,56,57,58] | |
| Saliva | >13–653 ng/mL (cutoff–IQR) | 0.04–14.9 ng/mL (min–max) | NA | NA | [36,38,39,40,59,60,61,62,63] | |
| Hair (min–max) | 0.08–2.49 ng/mg | 0.05–1.57 ng/mg | NA | NA | [23,35,64] | |
| 3HC | Urine (Mean (SD)) | 653.81 (62.30) µg/g cr | 60.79 (46.70) µg/g cr | NA | NA | [65] |
| NNN | Saliva (Mean (IQR)) | 118 (3.9–91) pg/mL | 5.3 (1.2–2.9) pg/mL a | NA | NA | [60] |
| NNK | Saliva (Mean (IQR)) | 6.6 (2.8–7.1) pg/mL | 4.5 (2.4–5.2) pg/mL a | NA | NA | [60] |
| NNAL | Urine | 80.9–405.5 pg/mL (Median range) | Low: 0.95–2.21 pg/mL (GM Range) High: 5.9–20.1 pg/mL (CI) | 2.7–6.7 pg/mL (GM range) | 0.86 pg/mg cr (CI) | [36,42,43,44,48,50,51,54,58,61,66] |
| Saliva (Mean (IQR)) | 3.2 (0.98–3.5) pg/mL | 1.3 (0.83–1.8) pg/mL a | NA | NA | [60] | |
| 1-OHNap, 2-OHNap | Urine | NA | 4587.6–6045.6 ng/L b | NA | 4466.1 ng/L (GM) | [57] |
| 2-OHFLu, 3-OHFlu, 9-OHFlu | Urine | NA | 571.0–824.8 ng/L b | NA | 439.9 ng/L (GM) | [57] |
| 1-OHPA, 2-OHPA, 3-OHPA | Urine | NA | 288.1–351.2 ng/L b | NA | 241.2 ng/L (GM) | [57] |
| 1-OHPyr | Urine | NA | 118.1–165.1 ng/L b | NA | 95.7 ng/L (GM) | [57] |
| Benzene | Urine (Median ± IQR) | NA | 596 ± 548 ng/L | Low: 282 ± 131 ng/L High: 314.5 ± 177 ng/L | 92.5 ± 90 ng/L | [67] |
| HPMM | Urine (Median (IQR)) | 1.63 (0.680–3.29) mg/g cr | NA | NA | 0.313 (0.231–0.451) mg/g cr | [55] |
| HMPA | Urine (IQR) | 1203–4898 pmol/mg cr | 1580–3964 pmol/mg cr | NA | NA | [68] |
| Cadmium | Urine (CI) | NA | 0.11–0.29 µg/L | NA | 0.097–0.12 μg/L | [46] |
| Whole blood c | NA | 1.07 µg/L | NA | 1.02 µg/L | [69] | |
| CO | Exhaled breath | >6–22.81 ppm (cutoff–mean) | 1.9–5.9 ppm (min–max) | NA | NA | [47,59] |
| COHb | Plasma (Mean (SD)) | 17.57% (8.79) | 1.2% (0.8) | NA | NA | [70] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres, S.; Merino, C.; Paton, B.; Correig, X.; Ramírez, N. Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 2693. https://doi.org/10.3390/ijerph15122693
Torres S, Merino C, Paton B, Correig X, Ramírez N. Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives. International Journal of Environmental Research and Public Health. 2018; 15(12):2693. https://doi.org/10.3390/ijerph15122693
Chicago/Turabian StyleTorres, Sònia, Carla Merino, Beatrix Paton, Xavier Correig, and Noelia Ramírez. 2018. "Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives" International Journal of Environmental Research and Public Health 15, no. 12: 2693. https://doi.org/10.3390/ijerph15122693