
Abstract
Summary
Adolescents with Down syndrome (DS) have poorer bone health than their peers without DS. Twenty-five adolescents with DS were randomly assigned to whole-body vibration training (WBV) or control groups. The results indicate that a 20-week WBV might be useful to improve subtotal bone mineral content and density in adolescents with DS.
Introduction
This study aims to determine the effects of 20 weeks of whole body vibration training (WBV) on bone mineral content (BMC), density (BMD), and structure variables in adolescents with Down syndrome (DS).
Methods
This randomized controlled trial of 25 adolescents (12–18 years) with DS (8 females) generated 2 non-equal groups, WBV group (n = 11) and CON group (n = 14). Using an efficacy analysis, the primary outcomes were BMC and BMD by dual-energy X-ray absorptiometry and the secondary were bone structure variables by peripheral quantitative computed tomography. A synchronous vibration platform (PowerPlate®) was used (3/week, 10 repetitions (30–60 s) 1-min rest, frequency of 25–30 Hz, and peak-to-peak displacement of 2 mm (peak acceleration 2.5–3.6 g)).
Results
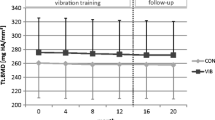
WBV group improved whole body BMC 2.8 %, 95 % CI [3.5, 2.1], subtotal area, BMC, and BMD by 2.8, 4.8, and 2 %, respectively, 95 % confidence intervals (CIs) [3.4, 2.1], [6.5, 3.1], and [2.8, 1.1], respectively (all, p < 0.05), showing group by time interactions in BMC and BMD (both p < 0.05). Lumbar spine BMC and BMD also increased in the WBV group by 6.6 and 3.3 % both p < 0.05, 95 % CIs [8.6, 4.7], and [4.9, 1.7], respectively. Regarding bone structure, WBV group showed improvements in tibial BMC at 4 % (2.9 %, 95 % CI [3.0, 2.8]) and in volumetric BMD (vBMD), cortical vBMD, and cortical thickness at 66 % of the radius (by 7.0, 2.4, and 10.9 %; 95 % CIs [7.4, 6.7], [2.6, 2.3], and [12.4, 9.3], respectively) (all, p < 0.05).
Conclusions
A 20-week WBV, with this protocol, might be useful to improve subtotal BMC and BMD in adolescents with DS.


Similar content being viewed by others


References
Bittles AH, Glasson EJ (2004) Clinical, social, and ethical implications of changing life expectancy in Down syndrome. Dev Med Child Neurol 46:282–286
No Authors (1993) Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650.
Sakadamis A, Angelopoulou N, Matziari C, Papameletiou V, Souftas V (2002) Bone mass, gonadal function and biochemical assessment in young men with trisomy 21. Eur J Obstet Gynecol Reprod Biol 100:208–212
Kao CH, Chen CC, Wang SJ, Yeh SH (1992) Bone mineral density in children with Down’s syndrome detected by dual photon absorptiometry. Nucl Med Commun 13:773–775
Baptista F, Varela A, Sardinha LB (2005) Bone mineral mass in males and females with and without Down syndrome. Osteoporos Int 16:380–388
Sepulveda D, Allison DB, Gomez JE, Kreibich K, Brown RA, Pierson RN Jr, Heymsfield SB (1995) Low spinal and pelvic bone mineral density among individuals with Down syndrome. Am J Ment Retard 100:109–114
González-Agüero A, Vicente-Rodríguez G, Moreno LA, Casajús JA (2011) Bone mass in male and female children and adolescents with Down syndrome. Osteoporos Int 22:2151–2157
Guijarro M, Valero C, Paule B, Gonzalez-Macias J, Riancho JA (2008) Bone mass in young adults with Down syndrome. J Intellect Disabil Res 52:182–189
Angelopoulou N, Souftas V, Sakadamis A, Mandroukas K (1999) Bone mineral density in adults with Down’s syndrome. Eur Radiol 9:648–651
González-Agüero A, Vicente-Rodríguez G, Gómez-Cabello A, Ara I, Moreno LA, Casajús JA (2012) A 21-week bone deposition promoting exercise programme increases bone mass in young people with Down syndrome. Dev Med Child Neurol 54:552–556
Ferry B, Gavris M, Tifrea C, Serbanoiu S, Pop AC, Bembea M, Courteix D (2014) The bone tissue of children and adolescents with Down syndrome is sensitive to mechanical stress in certain skeletal locations: a 1-year physical training program study. Res Dev Disabil 35:2077–2084
Reza SM, Rasool H, Mansour S, Abdollah H (2013) Effects of calcium and training on the development of bone density in children with Down syndrome. Res Dev Disabil 34:4304–4309
González-Agüero A, Vicente-Rodríguez G, Moreno LA, Guerra-Balic M, Ara I, Casajús JA (2010) Health-related physical fitness in children and adolescents with Down syndrome and response to training. Scand J Med Sci Sports 20:716–724
Rizzoli R, Bianchi ML, Garabedian M, McKay HA, Moreno LA (2010) Maximizing bone mineral mass gain during growth for the prevention of fractures in the adolescents and the elderly. Bone 46:294–305
Lips P (1997) Epidemiology and predictors of fractures associated with osteoporosis. Am J Med 103:3S–8S, discussion 8S-11S
Bauman AE (2004) Updating the evidence that physical activity is good for health: an epidemiological review 2000-2003. J Sci Med Sport 7:6–19
Vicente-Rodriguez G (2006) How does exercise affect bone development during growth? Sports Med 36:561–569
Matute-Llorente A, González-Agüero A, Gómez-Cabello A, Vicente-Rodríguez G, Casajús JA (2013) Effect of whole-body vibration therapy on health-related physical fitness in children and adolescents with disabilities: a systematic review. J Adolesc Health 54:385–396
Gomez-Cabello A, Gonzalez-Aguero A, Morales S, Ara I, Casajus JA, Vicente-Rodriguez G (2014) Effects of a short-term whole body vibration intervention on bone mass and structure in elderly people. J Sci Med Sport 17:160–164
Gomez-Cabello A, Ara I, Gonzalez-Aguero A, Casajus JA, Vicente-Rodriguez G (2012) Effects of training on bone mass in older adults: a systematic review. Sports Med 42:301–325
Dalen Y, Sääf M, Nyrén S, Mattsson E, Haglund-Akerlind Y, Klefbeck B (2012) Observations of four children with severe cerebral palsy using a novel dynamic platform. A case report. Adv Physiother 14:132–139
Ruck J, Chabot G, Rauch F (2010) Vibration treatment in cerebral palsy: a randomized controlled pilot study. J Musculoskelet Neuronal Interact 10:77–83
Gilsanz V, Wren TA, Sanchez M, Dorey F, Judex S, Rubin C (2006) Low-level, high-frequency mechanical signals enhance musculoskeletal development of young women with low BMD. J Bone Miner Res 21:1464–1474
Ward K, Alsop C, Caulton J, Rubin C, Adams J, Mughal Z (2004) Low magnitude mechanical loading is osteogenic in children with disabling conditions. J Bone Miner Res 19:360–369
Pitukcheewanont P, Safani D (2006) Extremely low-level, short-term mechanical stimulation increases cancellous and cortical bone density and muscle mass of children with low bone density: a pilot study. Endocrinologist 16:128–132
Soderpalm AC, Kroksmark AK, Magnusson P, Karlsson J, Tulinius M, Swolin-Eide D (2013) Whole body vibration therapy in patients with Duchenne muscular dystrophy—a prospective observational study. J Musculoskelet Neuronal Interact 13:13–18
González-Agüero A, Matute-Llorente A, Gómez-Cabello A, Casajús JA, Vicente-Rodríguez G (2013) Effects of whole body vibration training on body composition in adolescents with Down syndrome. Res Dev Disabil 34:1426–1433
Lam TP, Ng BK, Cheung LW, Lee KM, Qin L, Cheng JC (2012) Effect of whole body vibration (WBV) therapy on bone density and bone quality in osteopenic girls with adolescent idiopathic scoliosis: a randomized, controlled trial. Osteoporos Int 24:1623–1636
González-Agüero A, Vicente-Rodríguez G, Gómez-Cabello A, Ara I, Moreno LA, Casajús JA (2011) A combined training intervention programme increases lean mass in youths with Down syndrome. Res Dev Disabil 32:2383–2388
Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG (2012) CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg 10:28–55
Marfell-Jones M (2006) International standards for anthropometric assessment. International Society for the Advancement of Kinanthropometry. Potchefstroom, South Africa
Tanner JM, Whitehouse RH (1976) Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170–179
Gracia-Marco L, Ortega FB, Jimenez-Pavon D, Rodriguez G, Castillo MJ, Vicente-Rodriguez G, Moreno LA (2012) Adiposity and bone health in Spanish adolescents. The HELENA study. Osteoporos Int 23:937–947
Gomez-Bruton A, Gonzalez-Aguero A, Casajus JA, Vicente-Rodriguez G (2014) Swimming training repercussion on metabolic and structural bone development; benefits of the incorporation of whole body vibration or pilometric training; the RENACIMIENTO project. Nutr Hosp 30:399–409
González-Agüero A, Vicente-Rodríguez G, Gómez-Cabello A, Casajús JA (2013) Cortical and trabecular bone at the radius and tibia in male and female adolescents with Down syndrome: a peripheral quantitative computed tomography (pQCT) study. Osteoporos Int 24:1035–1044
Hoffman M, Schrader J, Applegate T, Koceja D (1998) Unilateral postural control of the functionally dominant and nondominant extremities of healthy subjects. J Athl Train 33:319–322
Szabo KA, Webber CE, Adachi JD, Tozer R, Gordon C, Papaioannou A (2011) Cortical and trabecular bone at the radius and tibia in postmenopausal breast cancer patients: a Peripheral Quantitative Computed Tomography (pQCT) study. Bone 48:218–224
Cohen J (1969) Statistical power analysis for the behavioural sciences. Academic Press, New York
Slatkovska L, Alibhai SM, Beyene J, Cheung AM (2010) Effect of whole-body vibration on BMD: a systematic review and meta-analysis. Osteoporos Int 21:1969–1980
Wu J (2013) Bone mass and density in preadolescent boys with and without Down syndrome. Osteoporos Int 24:2847–2854
Wren TA, Lee DC, Hara R, Rethlefsen SA, Kay RM, Dorey FJ, Gilsanz V (2010) Effect of high-frequency, low-magnitude vibration on bone and muscle in children with cerebral palsy. J Pediatr Orthop 30:732–738
Burrows M, Liu D, Moore S, McKay H (2010) Bone microstructure at the distal tibia provides a strength advantage to males in late puberty: an HR-pQCT study. J Bone Miner Res 25:1423–1432
Lynn HS, Lau EM, Au B, Leung PC (2005) Bone mineral density reference norms for Hong Kong Chinese. Osteoporos Int 16:1663–1668
O’Keefe K, Orr R, Huang P, Selvadurai H, Cooper P, Munns CF, Singh MA (2013) The effect of whole body vibration exposure on muscle function in children with cystic fibrosis: a pilot efficacy trial. J Clin Med Res 5:205–216
Acknowledgments
We gratefully acknowledge the help of all of the adolescents and their parents who participated in the study for their understanding and dedication to the project. Specials thanks are given to Fundación Down Zaragoza and Special Olympics Aragón for their support. The authors also thank Alex R. Jenkins from the Aberystwyth University for his work of reviewing the English style and grammar. This work was supported by “Ministerio de Ciencia e Innovación” “Plan Nacional I + D + i 2009–2011 (Project DEP 2009-09183).” This project has been co-financed by “Fondo Europeo de Desarrollo Regional” (MICINN-FEDER). AML received a Grant AP12-2854 from “Ministerio de Educación Cultura y Deportes.”
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Matute-Llorente, A., González-Agüero, A., Gómez-Cabello, A. et al. Effect of whole body vibration training on bone mineral density and bone quality in adolescents with Down syndrome: a randomized controlled trial. Osteoporos Int 26, 2449–2459 (2015). https://doi.org/10.1007/s00198-015-3159-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3159-1