
Abstract
Objectives:
The aim of this study was to investigate the pharmacological effects of long-term oral tadalafil treatment on the corpus cavernosum function in rats subjected to experimental spinal cord transection (SCT).
Methods:
Thirty young adult, male Sprague–Dawley rats were randomly divided into five groups (n=6, each), as follows: (1) Control, (2) Control surgery (Sham), (3) Tadalafil (Td), (4) Experimental SCT, and (5) SCT+Tadalafil (SCT+Td).
SCT rat model: after removal of T8-T9 spinal processes and laminates, a full-thickness scalpel incision was made in the spinal cord.
SCT+Td rat model: rats subjected to SCT were given tadalafil (5 mg kg−1, p.o.) for 4 weeks. Next, the penile cavernous tissues obtained by en bloc excision were trimmed free of the surrounding tissue to isolate cavernosal smooth muscle strips, which were then transferred into the isolated organ baths to investigate isometric tension changes in response to various bioactive agents and electrical field stimulation (EFS).
Results:
The relaxation response to acetylcholine at 0.01 mM concentration was significantly less in the SCT group compared with other groups. EFS-induced relaxation in the basal and precontracted cavernous tissue preparations was greater in the SCT+Td group than in the SCT group.
Conclusion:
This study demonstrated that long-term tadalafil administration preserves relaxation responses probably by affecting through the nitric oxide (NO)/cyclic guanosine monophosphate (cGMP) pathway in SCT-applied rats. This treatment strategy might preserve the erectile process and prevent the SCT-induced permanent damage in the cavernosal tissue.
Similar content being viewed by others


Introduction
Erectile dysfunction (ED) is defined as the inability to achieve and maintain penile erection necessary for sexual intercourse. Penile erection, a hemodynamic process produced by the interaction of the nervous system and local factors (nitric oxide, NO; soluble guanylyl cyclase, sGC; and cyclic guanosine monophosphate, cGMP), is characterized by the increase in penile arterial blood flow, the relaxation of sinusoidal smooth muscle tissue and the decrease in venous return.1
The penis is innervated by the autonomous and somatic nerves. Stimulation of the cholinergic and/or non-adrenergic/non-cholinergic (NANC) nerves induces smooth muscle relaxation. NANC nerves release NO, which diffuses into the neighboring smooth muscle cells and activates the intracellular enzyme sGC to cause an increase in the intracellular level of cGMP. cGMP induces smooth muscle relaxation. NO is also released from the arterial endothelial cells and sinusoidal underlying smooth muscle relaxation.2
The active mechanism of NO on the corpus cavernosum and penile arteries involves the stimulation of cGMP biosynthesis by activating sGC. An increased intracellular concentration of cGMP levels leads to the relaxation of the smooth muscle in the corpus cavernosum and penile arterioles. cGMP, similar to the other nucleosides, is metabolized by the enzyme phosphodiesterase (PDE). PDE-5 inhibitors prevent the breakdown of cGMP and support the formation of penile erection by causing sinusoidal smooth muscle relaxation.3
Brain modulation of the erection through neurophysiological evidence involving structures such as the medial preoptic area of hypothalamus, the paraventricular nucleus, the periaqueductal gray and through neuropharmacological evidence involving neurotransmitters. Erection parasympathetic center, located in the spinal cord segments S2–4, is the main mediator of erection; it affects vasodilation and opening of the arteriovenous shunts in the corpora cavernosa whereby erection is obtained. Sympathetic centers located in T11-L2 and sympathetic pathways are antierectile. The afferents transmitting penile sensation run in the pudendal nerve to the sacral center, and contraction of the perineal striated muscles improves penile rigidity. Relaxation of arterial and cavernous smooth muscle fibers, leading to the filling of the sinusoidal spaces with blood, is the local mechanism of erection. This is a result of parasympathetic/non-adrenergic non-cholinergic neural pathway activation and simultaneous inhibition of sympathetic outflow. Erection is a neurovascular event. Any disease or injury affecting the brain, spinal cord, cavernous and pudendal nerves would be hindered of the erection.4, 5
Approximately 10–20% of ED is of neurological origin. The neurogenic ED is classified into three groups: supraspinal, spinal (sacral and suprasacral) and peripheral. The main causes of neurogenic ED include stroke, Alzheimer’s disease, spinal cord injury (SCI), spinal lesions, pelvic injury, pelvic surgery, diabetic neuropathy and multiple sclerosis. Almost 50% of ED cases resulted from SCI. Depending on the level of SCI, reflexogenic erection and/or psychogenic erection may occur in the patients.6
As sexual function is associated with the innervation of the reproductive system, defining the neurological level of SCI is important to estimate the residual sexual capacity. The spinal cord can be classified into three sections, owing to the level of the spinal centers having a role in sexual function, as T10 and above, T11-L2 (the sympathetic center) and conus–cauda (the sacral parasympathetic center as follows).
T10 and above: Local stimulation of the genital organs can be answered. However, the psychogenic erection cannot occur.
From T11-L2: Erection was expected with genital stimulation, as well as with psychogenic stimulation.
Conus–cauda (sacral lesion of the way): Conus–cauda comprise the conus terminalis and the cauda equina. Usually, any type of erection does not occur. In the first group, protection of psychogenic erection is more frequent than the second group.7, 8
In this study, we aimed to investigate the functional changes due to spinal cord transection (SCT) in the corpus cavernosum tissue, and to show the possible pharmacological effects of long-term oral tadalafil treatment on the cavernosal function in an experimental SCT model in rats. The objective of this work was also to provide reliable data to suggest whether long-term tadalafil treatment is only a symptomatic approach or might be curative in SCT-induced ED. Generally, patients believed that ‘long-term’ medication means chronic medication for more than 2 or 3 months. The duration of treatment varies according to the etiology, and ranges from 2 to 24 months.9 In the other study, the experimental period usually ranged from 4 to 8 weeks for long-term PDE5I treatment rat models.10, 11
Materials and methods
After being approved by the Baskent University Research Council and the Ethical Committee of Research on Animals (01/07/2010-DA10/15), this study was conducted at Baskent University Experimental Animal Research Center.
Thirty adult, male Sprague–Dawley rats weighing 250–300 g were used in the study. The rats were housed in polycarbon cages at 20±2 °C, in a humidity-controlled environment (%50±10) with a 12-h light/dark cycle, preoperatively and postoperatively. The rats were randomly and equally assigned to five groups (n=6, each): (1) Control (C), (2) Sham (S), (3) Tadalafil-administered (Td), (4) Experimental SCT-applied and (5) SCT-applied and Tadalafil-administered (SCT+Td). The rats received enrofloxacin (10 mg kg−1 per day, intramuscularly) before the surgery and for 3 days after the surgery. The experimental process is summarized in Table 1.
Experimental SCT model
The rats in S, SCT and SCT+Td groups were anesthetized intraperitoneally by ketamine (60 mg kg−1) and xylasine (7 mg kg−1). After the anesthesia reached the level necessary for surgery, a dorsal midline skin incision was made between T7 and T10 levels. After the spinal processes and laminates of T8–T9 were removed, a full-thickness incision was made on the spinal cord with a scalpel.12
Long-term tadalafil administration
Tadalafil (5 mg kg−1 per day) was administered to the rats with an orogastric catheter for 4 weeks.
After 4 weeks, the penises were resected and corpus cavernosum strips were prepared.
Corpus cavernosum preparation
Having the penis defined, a midline incision was performed on the prepicium. Cavernous tissues were dissected gently to the level of crus penis. The penis was resected en bloc from the proximal of the cruses, and it was then taken into the dissection plate containing ice-cold Krebs-Henseleit solution.
Isolated organ bath experiments
The corpus cavernosum tissue was trimmed free of the surrounding connective tissue and prepared for isolated organ bath (IOB) experiments. Next, the corpus cavernosum strips were transported to the IOB system. Tissues were allowed to equilibrate for 60 min without adding any test agents into the IOBs under an initial resting tension of 1 g to get the optimal isometric responses. The isometric contraction and relaxation responses received via force-displacement transducers were amplified, evaluated and recorded by a computerized physiological data acquisition system. All of the isometric responses were normalized to the contraction in response to initial phenylephrine (PE; 10−4 M) administration in each strip individually.13
Electrical field stimulation
Each cavernous tissue strip was exposed to electrical field stimulation (EFS) through two platinum electrodes, between which the strip was mounted. EFS was applied to mimic the nerve-mediated excitation-response coupling of the corpus caverosum tissue by stimulating the intramural nerves within the tissue. The contraction and relaxation responses induced by EFS were evaluated. EFS was applied initially to the resting tissue, and then three times to the strips precontracted with PE (10−4 M), either in the presence or absence of nitro-L-arginine methyl ester (L-NAME), propranolol and atropine+guanethidine incubations. The latter antagonists were used to exclude the possibility of the involvement of cholinergic and/or adrenergic systems in the responses.
Isometric contraction experiments
The logarithmic concentration–contraction curves were obtained by the cumulative administration of PE (10−9–10−3 M) to the corpus cavernosum strips.
Isometric relaxation experiments
The relaxations, if any, in response to acetylcholine (ACh; 10−7–10−5 M) and L-arginin (L-Arg; 10−7–10−3 M) were investigated in the corpus cavernosum strips precontracted by PE (10−4 M).
Involvement of nitric oxide system in the isometric responses
To investigate the involvement of nitric oxide (NO)-guanylate cyclase system in the EFS-induced relaxation responses, the experimental protocol was repeated after the corpus cavernosum strips were incubated for 15 min with the NO synthase inhibitor L-NAME (10−3 and 10−4 M).
Statistical analysis
‘SPSS 15.0 for Windows’ (SPSS Inc, Chicago, Il, USA) package program was used for statistical analysis. The data, expressed as mean±s.d., were analyzed with Mann–Whitney U-test for dual comparions and with Kruskal–Wallis analysis of variance test for multiple comparisons. P<0.05 was considered statistically significant.
Results
Isometric contraction responses
PE-induced sigmoidal concentration-response curves were almost the same in all of the groups, indicating that neither surgery nor tadalafil treatment affected the contractile process in the corpus cavernosum tissue (Figure 1).

Concentration–contraction curves obtained in response to PE administration in rat-isolated corpus cavernosum strips.
Isometric relaxation responses
There was no significant difference in the ACh relaxation responses between the groups (P>0.05). The SCT group significantly impaired the relaxation response to ACh at 10−5 M concentration compared with the other groups (P<0.05). In the SCT+Td group, significantly more relaxation response to ACh was observed compared with the SCT group (P<0.05). There were no differences between SCT+ Td, sham and control group relaxation responses to ACh. Tadalafil treatment increased the relaxant response to ACh at 10−5 M, but it was not significant (P>0.05) (Figure 2).

ACh-induced concentration-relaxation responses in rat-isolated corpus cavernosum strips precontracted with 10−4 M PE.
L-NAME (10−3 M) incubation blunted the ACh-induced relaxations in all of the groups significantly, indicating the involvement of NO synthase in ACh relaxations in the corpus cavernosum tissue (P<0.05).
L-Arg induced concentration-dependent relaxations in all of the groups. L-NAME (10−3 M) incubation caused most inhibition in the SCT group. Better relaxation response was observed in SCT-applied rats with Tadalafil treatment. However, none of the groups were significantly different from the others (Figure 3).

The effect of L-NAME (10−3 M) incubation on L-arginin (L-Arg)-induced concentration-dependent relaxation responses in rat-isolated corpus cavernosum strips precontracted with 10−4 M PE.
EFS responses
EFS induced a triphasic response pattern in rat-isolated corpus cavernosum tissue, regardless of whether it was at baseline or was precontracted with PE (Figure 4): a spike-shaped initial phasic contraction, followed by a tonic relaxation, and then a tonic contraction triggered by the stimulus withdrawal (off response).

The sample tracing displaying the triphasic isometric response pattern to EFS application in the rat-isolated corpus cavernosum strips precontracted with PE (10−4 M).
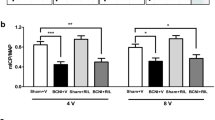
Isolated corpus cavernosum strips from tadalafil-treated, SCT-applied rats showed more relaxation response due to EFS at baseline (in the absence of any test agents in the IOB) in comparison with that of the SCT group (P<0.05) There was no significant difference between groups regarding the relaxation responses due to EFS in precontracted strips. However, the SCT+Td group showed significantly more relaxation in response to EFS than the SCT group. In addition, tadalafil treatment caused more marked relaxations in response to EFS than the other groups (P<0.05).
L-NAME incubation inhibited the EFS-induced relaxation responses in all of the groups, whereas atropine+guanethidine or propranolol incubations did not cause a prominent effect on the relaxant responses, indicating the involvement of the NANC system in the functional activity examined (Figure 5).

The role of nitrergic, adrenergic and cholinergic nerves and beta adrenergic receptors in the EFS-induced relaxation responses in rat-isolated corpus cavernosum strips.
Discussion
In the present study, the effect of long-term tadalafil treatment was investigated in the corpus cavernosum tissues isolated from SCT-applied rats with the help of certain pharmacological agents and EFS, which were applied to evaluate the functional status of the cavernous smooth muscle tissue. SCT significantly impaired the relaxation response to ACh at 10−5 M concentration compared with other groups. On the other hand, tadalafil treatment caused more marked relaxations in response to EFS than the other groups.
Male sexual responses are reflexes mediated by the spinal cord and modulated by neural circuitries involving both the peripheral and central nervous system. SCI-induced ED occurs as a result of upper motor neuron damage. Several studies have shown that while the brain interacts with the reflexes to allow perception of sexual sensations, penile reflexes can occur despite complete transections of the spinal cord. Thoracic spinal block did not reverse the complete abolition of reflexive erections.14, 15 The formation of thoracolumbar synaptic connections provides the reflex erection path in the sacral SCI. Acute SCI permits phasic penile erection, and these sexual reflexes can be observed during several weeks in the rat without significant changes.16
Shin et al.17 reported that apoptosis, collagen deposition, smooth muscle cell loss and fibrosis were increased in the corpus cavernoum tissue specimens obtained by percutaneous biopsy from 10 SCI-induced ED patients. The authors also suggested that the patients might benefit from early pharmacotherapy (PDE-5 inhibitors) to prevent this irreversible injury. Treatment should be initiated immediately after SCI.
The findings of the present study supported this suggestion, that is, initiating a long-term PDE-5 inhibitor treatment as early as possible may prevent the irreversible damage in the cavernous tissue due to SCT. It has been suggested that SCI inhibits erection development by affecting the NO release from the parasympathetic and NANC nerve terminals.6
Hannan et al.18 showed that inhibition of Rho-kinase improves erectile function associated with bilateral cavernous nerve injury by increasing NO signaling and decreasing penile apoptosis in a rat model of cavernous nerve damage.
The major change in the dosing scheme of PDE-5 inhibitors since their emergence to the clinical use has been the definition and recommendation of their long-term (chronic) use.19 This regimen aims to improve the self-esteem of the patient by providing spontaneous sexual activity. It was shown that long-term PDE-5 inhibitor treatment caused an increase in IIEF scores by 10.8% at the end of the 2-year follow-up period.20
Tadalafil is used at 2.5–5 mg daily doses. It has been proposed that daily use of tadalafil induces regular erections and increases penile blood flow, which is likely to prevent the physiopathological process leading to fibrosis development.20, 21
The detumescence of the erected penis is provided by adrenergic nerves. PE activates the α1 adrenoceptors on the penile smooth muscle cell membrane.22 We did not observe any difference among the groups in response to PE administration regarding the concentration–contraction curves. We therefore suggest that contractile functions of the cavernous smooth muscle are preserved even in SCT-applied rats.
In the present study, the relaxation responses to L-Arg were smaller in the SCT group, which were improved by long-term tadalafil treatment, indicating the impairing effect of spinal cord damage on the relaxation function of corpus cavernosum, which was reversed by tadalafil. It might be suggested that tadalafil-mediated recovery of the relaxation responses in SCT-applied rat corpus cavernosum tissue is due to intracellular cGMP accumulation. As L-NAME incubation did not elicit any significant difference in the ACh-induced relaxations among the groups, ACh is likely to act on the endothelial NO pathway.
The greater relaxations in the cavernosal smooth muscle strips that we observed in response to ACh administration indicated that long-term tadalafil treatment may contribute to the erectile function, and neither receptor desensitization nor mediator depletion occurs as a consequence of long-term tadalafil use.
L-NAME incubation resulted in a decrease in the relaxation response to L-Arg only in the SCT group significantly. On the other hand, long-term tadalafil treatment led to an increase in these relaxations. This finding indicated that long-term tadalafil treatment probably helped the tissue to preserve the NO/cGMP pathway after SCT surgery.
We observed in SCT-applied rats that long-term tadalafil treatment significantly reversed the decrease in EFS-induced relaxations in isolated corpus cavernosum smooth muscle preparations, regardless of being either at baseline or precontracted. Moreover, even while under antagonist incubation, the cavernosal strips isolated from tadalafil-treated rats relaxed more in response to EFS applied at baseline or on precontraction. It was reported that nerve injury resulted in a marked reduction in the responses induced by EFS in rats, probably because of the impairment in NO synthesis and/or release at the nerve terminal.23
Incubating the cavernosal strips with atropin+guanetidin cocktail or propranolol did not produce a significant difference from the naive relaxations in response to EFS, suggesting that neither adrenergic and cholinergic nerves nor beta adrenoceptors are of major importance in these relaxations, but the NANC system is. In support of this, L-NAME incubation significantly decreased the EFS-induced relaxations, indicating the role of NANC system and NO synthesis in this erection-mimicking model.
In the present study, EFS-induced relaxation responses were significantly greater in the long-term tadalafil-treated rats. This might be due to the cGMP preserving the effect of tadalafil, as EFS-induced increase in NO production might subsequently enhance the amount of cGMP in the corpus cavernosum.
Conclusion
Our findings revealed that long-term tadalafil treatment in SCI-induced ED saved the relaxation function of rat corpus cavernosum by preserving the availability of the NO/cGMP pathway. To prevent the development of permanent damage in the cavernous tissue and to ensure the patient’s sexual rehabilitation, long-term tadalafil treatment appears to be necessary.
Data archiving
There were no data to deposit.
References
Lue TF . Erectile dysfunction. N Engl J Med 2000; 342: 1802–1813.
Jin HR, Chung YG, Kim WJ, Zhang LW, Piao S, Tuvshintur B . A mouse model of cavernous nerve injury-induced erectile dysfunction: functional and morphological characterization of the corpus cavernosum. J Sex Med 2010; 7: 1733–1758.
Kang KK, Ahn GJ, Ahn BO, Yoo M, Kim WB . DA-8159, a new PDE5 inhibitor, induces penile erection in conscious and acute spinal cord injured rabbits. Eur Urol 2003; 43: 689–695.
Biering-Sørensen F, Sønksen J . Sexual function in spinal cord lesioned men. Spinal Cord 2001; 39: 455–470.
Jannini EA, McCabe MP, Salonia A, Montorsi F, Sachs BD . Organic vs. psychogenic? The Manichean diagnosis in sexual medicine. J Sex Med 2010; 7: 1726–1733.
Jung JY, Kim SK, Kim BS, Lee SH, Park YS . The penile erection efficacy of a new phosphodiesterase type 5 inhibitor, mirodenafil (SK3530), in rabbits with acute spinal cord injury. J Vet Med Sci 2008; 70: 1199–1204.
Rizio N, Tran C, Sorenson M . Efficacy and satisfaction rates of oral PDE5is in the treatment of erectile dysfunction secondary to spinal cord injury: A review of literature. J Spinal Cord Med 2012; 35: 219–228.
Lagoda G, Jin L, Lehrfeld TJ, Liu T, Burnett AL . FK506 and sildenafil promote erectile function recovery after cavernous nerve injury through antioxidative mechanisms. J Sex Med 2007; 4 (4 Pt 1): 908–916.
Tang Y, Gan Y, He L . Recent progression for application of tadalafil. Sci Res Essays 2011; 6: 6769–6773.
Gur S, Kadowitz PJ, Gurkan L, Chandra S . Chronic inhibition of nitric-oxide synthase induces hypertension and erectile dysfunction in the rat that is not reversed by sildenafil. BJU Int 2010; 106: 78–83.
De Young LX, Domes T, Lim K, Carson J, Brock GB . Endothelial rehabilitation: the impact of chronic PDE5 inhibitors on erectile function and protein alterations in cavernous tissue of diabetic rats. Eur Urol 2008; 54: 213–220.
Allen AR . Surgery of experimental lesion of spinal cord equivalent to crush injury of fracture dislocation of spinal column. Preliminatory report. JAMA 1911; 57: 877–880.
Lin RJ, Wu BN, Lo YC, Shen KP, Lin YT, Huang CH et al. KMUP-1 relaxes rabbit corpus cavernosum smooth muscle in vitro and in vivo: involvement of cyclic GMP and K+ channels. Br J Pharmacol 2002; 135: 1159–1166.
Sachs BD, Bitran D . Spinal block reveals roles for brain and spinal cord in the mediation of reflexive penile erections. Brain Res 1990; 528: 99–108.
Lombardi G, Nelli F, Celso M, Mencarini M, Del Popolo G . Treating erectile dysfunction and central neurological diseases with oral phosphodiesterase type 5 inhibitors. Review of the literature. J Sex Med 2012; 9: 970–985.
Lavrov I, Gerasimenko YP, Ichiyama RM, Courtine G, Zhong H, Roy RR . Plasticity of spinal cord reflexes after a complete transection in adult rats: relationship to stepping ability. J Neurophysiol 2006; 96: 1699–1710.
Shin TY, Ryu JK, Jin HR, Piao S . Increased cavernous expression of transforming growth factor-β1 and activation of the Smad signaling pathway affects erectile dysfunction in men with spinal cord ınjury. J Sex Med 2010; 4: 1743–1762.
Hannan JL, Albersen M, Kutlu O, Gratzke C, Stief CG, Burnett AL et al. Inhibition of Rho-kinase Improves erectile function, ıncreases nitric oxide signaling and decreases penile apoptosis in a rat model of cavernous nerve ınjury. J Urol. 2013; 189: 1155–1161.
Donatucci CF, Wong DG, Giuliano F, Glina S, Dowsett SA, Watts S . Efficacy and safety of tadalafil once daily: considerations for the practical application of a daily dosing option. Curr Med Res Opin 2008; 24: 3383–3392.
Porst H, Rajfer J, Casabé A, Feldman R, Ralph D, Vieiralves LF . Long-term safety and efficacy of tadalafil 5 mg dosed once daily in men with erectile dysfunction. J Sex Med 2008; 5: 2160–2169.
Eardley I, Donatucci C, Corbin J, El-Meliegy A, Hatzimouratidis K, McVary K . Pharmacotherapy for erectile dysfunction. J Sex Med. 2010; 7: 524–540.
Mulhall JP, Land S, Parker M, Waters WB, Flanigan RC . The use of an erectogenic pharmacotherapy regimen following radical prostatectomy recovery of spontaneous erectile function. J Sex Med 2005; 2: 532–542.
Borisoff JF, Elliott SL, Hocaloski S, Birch GE . The development of a sensory substitution system for the sexual rehabilitation of men with chronic spinal cord injury. J Sex Med 2010; 7: 3647–3658.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Toksoz, S., Erdem, S., Peskircioglu, C. et al. The effect of long-term oral tadalafil treatment on corpus cavernosum function in an experimental spinal cord transection rat model. Spinal Cord 51, 663–667 (2013). https://doi.org/10.1038/sc.2013.61
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2013.61
Keywords
This article is cited by
-
Mesenchymal stem cell therapy improves erectile dysfunction in experimental spinal cord injury
International Journal of Impotence Research (2020)
