
Abstract
Aims/hypothesis
A retrospective analysis of pooled data from twelve placebo-controlled trials was conducted to characterise the efficacy and safety of tadalafil for the treatment of erectile dysfunction in men with diabetes compared with that in men without diabetes.
Methods
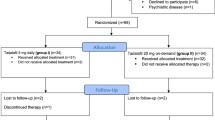
Patients were randomly allocated to tadalafil 10 mg, 20 mg, or placebo, taken as needed for 12 weeks. The study population comprised 637 men with diabetes (mean age 57 years) and 1681 men without diabetes (mean age 56 years).
Results
At baseline, patients with diabetes had more severe erectile dysfunction than patients without diabetes, with mean International Index of Erectile Function (IIEF) erectile function domain scores of 12.6 and 15.0 respectively (p<0.001). Compared with placebo, tadalafil 10 mg and 20 mg improved all primary efficacy outcomes in both patient groups (p<0.001). Men with diabetes receiving tadalafil 20 mg experienced a mean improvement of 7.4 in their IIEF erectile function domain score against baseline versus 0.9 for placebo (p<0.001). This group reported on average that 53% of their attempts at intercourse were successful, compared with 22% for placebo (p<0.001 for the change from baseline). Baseline IIEF erectile function domain scores correlated inversely with baseline HbA1c levels. The responses to tadalafil were similar regardless of levels of baseline glycaemic control, diabetic therapy received, or previous use of sildenafil.
Conclusions/interpretation
Despite more severe baseline erectile dysfunction in men with diabetes, tadalafil was efficacious and well tolerated in this population. As reported for other phosphodiesterase 5 inhibitors, the response to tadalafil was slightly lower in men with diabetes than in men without diabetes.
Similar content being viewed by others


Introduction
Diabetes mellitus is associated with accelerated large vessel atherosclerosis, microvascular arterial disease, autonomic neuropathy, dyslipidaemia, concomitant hypertension and prominent endothelial dysfunction [1]. All of these conditions contribute to erectile dysfunction, and in men with diabetes, the risk of erectile dysfunction is approximately four-fold higher than in men without diabetes [2, 3]. Erectile dysfunction in men with diabetes is also more severe and less responsive to therapy than in men without diabetes [4].
Nitric oxide (NO) released in response to sexual stimulation relaxes penile vascular smooth muscle by increasing intracellular concentrations of cyclic guanosine 3′,5′-monophosphate (cGMP) [5, 6]. Vasodilation of erectile tissues allows the sinusoidal spaces to fill with blood, resulting in the attainment and maintenance of an erection. This process is reversed by phosphodiesterase type 5 (PDE5), the major PDE in penile cavernosal smooth muscle that is responsible for cGMP degradation [7]. PDE5 inhibitors (e.g. tadalafil, sildenafil citrate and vardenafil) enhance the downstream effect of NO by preventing cGMP degradation [8]. Although these drugs have been effective in men with varied causes and severity of erectile dysfunction, the response to PDE5 inhibition depends on the baseline quality of pudendal blood flow and the capacity of the vascular endothelial cell and pudendal nerve to release NO during sexual stimulation [9, 10, 11]. In patients with diabetes, hyperglycaemia impairs NO release by endothelial cells and the pudendal nerve [12, 13, 14]. Endothelial dysfunction in diabetes may also contribute significantly to the pathogenesis of erectile dysfunction and cardiovascular disease [15, 16, 17]. Thus, the combination of pronounced vascular insufficiency, autonomic neuropathy and endothelial dysfunction leads to more severe erectile dysfunction in men with diabetes, and these patients are less responsive to PDE5 inhibition than patients in an age-matched cohort without diabetes [4].
To determine how baseline characteristics and treatment outcomes in patients with erectile dysfunction differed in men with and without diabetes, we conducted a retrospective analysis of data from the twelve primary placebo-controlled tadalafil clinical efficacy studies that have been completed to date.
Subjects and methods
Study design
The twelve randomised, double-blind, placebo-controlled parallel group studies in our analysis were conducted in accordance with the ethical principles of the Declaration of Helsinki at 188 outpatient centres in North America, South America, Europe, Asia and Australia from November 1999 to February 2003 (Table 1). One study enrolled only men with erectile dysfunction and diabetes; the remaining 11 studies included men with diverse aetiologies of erectile dysfunction. Informed consent was obtained from all subjects. A screening visit included medical history, physical examination, laboratory safety tests and an electrocardiogram. Patients entered a 4-week, treatment-free, run-in period, during which baseline severity of erectile dysfunction was established. Eligible patients were then randomly allocated to a 12-week, double-blind treatment period with placebo or a fixed dose of tadalafil. For the purposes of this analysis, the diagnosis of diabetes mellitus was based on the patient’s medical history. In 606 of 637 patients (95%), the diagnosis of diabetes was confirmed by the use of concomitant hypoglycaemic medications, elevated HbA1c or elevated random glucose levels (based upon diagnostic criteria of the American Diabetes Association).
Study population
Eligible men were 18 years old and older, had a minimum 3-month history of erectile dysfunction (defined as a consistent change in the quality of erection that adversely affects the patient’s satisfaction with sexual intercourse), were in a stable heterosexual relationship, and agreed not to use any other erectile dysfunction treatment from the run-in period until the final study visit. Patients were excluded from the study if receiving nitrates, or if they had a recent history of serious unstable cardiovascular condition, stroke or spinal cord injury. Additional exclusion criteria included: uncontrolled blood pressure, HbA1c 13% or higher, clinically significant renal or hepatic insufficiency, or history of radical prostatectomy or other pelvic surgery with subsequent failure to achieve an erection. Patients who had undergone bilateral nerve-sparing prostatectomy were eligible, irrespective of their ability to achieve an erection. In addition, patients with stable cardiovascular conditions, multiple cardiovascular risk factors, diabetic retinopathy, urinary microalbuminuria, or diabetic neuropathy were eligible for enrollment. Sildenafil non-responders were excluded from most studies.
Study drug
Placebo and tadalafil (10 and 20 mg doses) were studied in this pooled analysis. Patients were instructed to take the study drug with water prior to expected sexual activity, but no more than once per day. No restrictions were placed on food or alcohol intake, or timing of sexual activity relative to dosing. Study drugs were provided at no cost to the patient by Lilly ICOS LLC.
Study evaluations
Erectile function was measured at the end of the run-in period and every 4 weeks during the treatment period using the International Index of Erectile Function (IIEF) [18]. The Sexual Encounter Profile (SEP) patient diary was also completed after every sexual attempt. The IIEF erectile function domain consists of six questions regarding erection frequency, erection firmness, penetration ability, maintenance frequency, maintenance ability, and erection confidence, with a possible total score ranging from 1 to 30. The change from baseline to endpoint in the IIEF erectile function domain score and in the percentage of ‘yes’ responses to SEP questions 2 (vaginal penetration) and 3 (intercourse success) were the co-primary efficacy endpoints. Secondary endpoints included the proportion of ‘yes’ responses to a global assessment question (GAQ), namely “Has the treatment you have been taking during this study improved your erections?”. This question was answered at the end of the treatment period or upon early discontinuation. Safety evaluations included routine laboratory tests (serum chemistry, haematology and urinalysis), adverse event collection, vital sign determination, and physical examination.
Statistical analysis
Efficacy analyses were conducted on an intent-to-treat basis and included patients who had a baseline and at least one post-baseline measurement. The IIEF erectile function domain was analysed using the last-observation-carried-forward convention. The baseline and endpoint score for each SEP question was the patient’s percentage of ‘yes’ responses to that question during the run-in and post-baseline periods respectively. Changes in proportions were treated as continuous outcomes. Analysis of covariance (ANCOVA) models of combined data from twelve studies were used with terms for study, treatment group, and baseline value, with a baseline by treatment group interaction term if significant (p<0.10). Pairwise comparisons of active doses versus placebo were based on least-squares means.
Analysis of the percentage of patients responding ‘yes’ to the GAQ included all patients who answered the question at the end of treatment or upon early discontinuation. Analysis of the percentage of patients attaining an erectile function domain score of 26 or higher at endpoint included all patients with an erectile function domain score of less than 26 at baseline and at least one post-baseline erectile function domain score. The GAQ and the percentage of patients attaining an erectile function domain score of 26 or higher at endpoint were analysed using a logistic regression model with terms for study, treatment group, and baseline erectile function domain score. The effect of diabetes on mean change in IIEF erectile function domain and SEP question 3 scores with tadalafil treatment was assessed by the significance of the subgroup by treatment interaction term in an ANCOVA model. The ANCOVA model included terms for study, subgroup, treatment group, subgroup by treatment group interaction, baseline efficacy score, and baseline efficacy score by treatment group interaction if significant (p<0.10). The test of whether the effect of tadalafil relative to placebo varied according to baseline HbA1c, type of diabetic therapy (insulin, oral medication only, or no medication), and previous sildenafil treatment was analysed in a similar manner.
Analysis of SEP question 3 by time from dose to attempt included all patients with at least one attempt made within the respective time interval and was analysed in the same manner as the overall analysis. Analyses were conducted using the SAS statistical package (version 8.2, SAS Institute, Cary, N.C., USA).
Treatment-emergent adverse events, defined as events that first occurred or worsened after randomisation, were summarised by the preferred terms in the Medical Dictionary for Regulatory Activities (MedDRA version 5; MedDRA MSSO, Reston, Va., USA). Baseline and demographic characteristics of diabetic and non-diabetic patient subpopulations were compared by ANOVA (adjusting for study) for continuous variables and the Cochran–Mantel–Haenszel test (adjusting for study) for categorical variables.
Results
Demographics
The mean patient age was 57±9 years for the patients with diabetes and 56±11 years for the patients without diabetes (p=0.26; Table 2). Mean body mass index (28.1 kg/m2) for patients with diabetes was higher than for patients without diabetes (27.2 kg/m2, p<0.001). Comorbid conditions that were more common in patients with diabetes included hypertension, hyperlipidaemia and coronary artery disease. Mean HbA1c levels were 8.1±1.5% for patients with diabetes (normal range: 4.3–6.1%). Mean baseline IIEF erectile function domain scores and all additional measures of baseline erectile dysfunction severity were well balanced in all treatment groups for patients with and without diabetes.
Based upon the IIEF questionnaire and SEP patient diary recordings, patients with diabetes had more severe erectile dysfunction at baseline than non-diabetic counterparts (Table 2). The mean IIEF erectile function domain in patients with diabetes was 12.6, compared to 15.0 in the population without diabetes (p<0.001). Patients with diabetes had a mean 17% success rate for intercourse attempts during the treatment-free run-in period, versus 24% for patients without diabetes (p<0.001). Based on IIEF erectile function domain scores [19], 47% of patients with diabetes and 31% of patients without diabetes had severe erectile dysfunction at baseline.
Efficacy
Compared with placebo, tadalafil improved erectile function in diabetic and non-diabetic men with erectile dysfunction (Table 3, Fig. 1) (p<0.001 for all primary and secondary efficacy endpoints). The mean improvement in IIEF erectile function domain score for men with diabetes was 6.2 for tadalafil 10 mg and 7.4 for tadalafil 20 mg, versus 0.9 for placebo (p<0.001 for both dose groups). For men without diabetes, the mean change was slightly greater: 6.7 for tadalafil 10 mg and 8.9 for tadalafil 20 mg, versus 0.8 for placebo (both p<0.001, interaction p value=0.006). The mean percentage of attempts resulting in successful completion of sexual intercourse (SEP question 3) also increased significantly in patients treated with tadalafil 10 and 20 mg, with mean changes from baseline of 30% and 37% respectively for men with diabetes, and 35% and 47% for men without diabetes (all p<0.001 vs placebo, interaction p value=0.028).

Tadalafil treatment in diabetic and non-diabetic patients. a. IIEF erectile function domain. b. Successful penetration (SEP question 2). c. Successful intercourse completion (SEP question 3). Bars represent mean endpoint values after 12 weeks of treatment; dashed lines represent mean baseline values for each of the three coprimary endpoints. **p<0.001 compared to placebo. Open bars: placebo; light grey bars: tadalafil 10 mg; dark grey bars: tadalafil 20 mg
The mean proportion of successful intercourse attempts (SEP question 3) with tadalafil 20 mg was 53% for patients with diabetes, compared with 22% in patients receiving placebo, and 71% and 33% for patients without diabetes taking tadalafil 20 mg and placebo respectively. A greater proportion of men, both with and without diabetes, who were receiving tadalafil indicated that the treatment improved their erections (GAQ) compared with patients assigned to placebo treatment (Table 3).
Baseline IIEF erectile function scores correlated inversely with baseline HbA1c levels in diabetic patients with erectile dysfunction (Pearson’s r=−0.14; p<0.001); the mean IIEF scores at baseline in patients with good (HbA1c <7.0%), fair (HbA1c 7.0–9.5%), or poor (HbA1c >9.5%) glycaemic control were 14.1, 12.4, and 11.5 respectively. Similarly, during the treatment-free period, the mean rates of successful intercourse in patients with good, fair, or poor glycaemic control were 21%, 17% and 12% respectively. Despite the more severe baseline erectile dysfunction associated with poor glycaemic control, tadalafil treatment significantly improved erectile function and intercourse success in each patient subgroup, except for the erectile function domain score in the 10-mg tadalafil group with poor glycaemic control (Fig. 2). The effect of tadalafil relative to placebo was not significantly influenced by baseline HbA1c levels (interaction p values: p=0.52 for erectile function domain score, p=0.70 for SEP question 3). Tadalafil treatment improved erectile function in patients taking oral hypoglycaemic medications, insulin, or neither (Table 4). The effect of tadalafil relative to placebo was not significantly influenced by type of diabetic therapy (interaction p values: p=0.32 for IIEF erectile function domain score, p=0.90 for SEP question 3).

Tadalafil treatment efficacy in diabetic patients as a function of glycaemic control. a. IIEF erectile function domain. b. Successful intercourse completion (SEP question 3). Bars represent mean endpoint values after 12 weeks of treatment; dashed lines represent mean baseline values. *p<0.05; ** p<0.001 compared to placebo. Open bars: placebo; light grey bars: tadalafil 10 mg; dark grey bars: tadalafil 20 mg
Patients who, in the opinion of the investigator, had had prior ineffective treatment with sildenafil were excluded from nine of the twelve studies. Among men with diabetes, response to tadalafil in these studies was similar between patients previously treated with sildenafil (presumptive sildenafil responders, based upon study entry criteria) and those not previously treated with sildenafil. For tadalafil 20 mg, the mean change from baseline in IIEF erectile function domain score was 6.8 for men previously treated with sildenafil (n=134) and 8.4 for patients with no prior sildenafil use (n=89), compared with 0.8 (n=57) and 1.7 (n=34) in the respective placebo groups (both p<0.001 versus placebo, interaction p-value=0.80). Results for the other coprimary endpoints were similar.
The success rate of intercourse attempts was relatively stable over time at time intervals of up to 36 hours after treatment with tadalafil (Fig. 3). The mean per-patient percentage of successful intercourse attempts with tadalafil 20 mg ranged from 50 to 63% at time intervals from 0.5 to 36 hours, versus 22 to 30% for placebo and 45 to 61% for tadalafil 10 mg.

Effects of tadalafil treatment on successful intercourse completion (SEP question 3) over time in diabetic patients. Bars represent mean per-patient success; dashed lines represent mean baseline values. * p<0.05; **p<0.001 compared to placebo. The number in each bar represents the number of patients having at least one attempt at intercourse in the respective time interval. Open bars: placebo; light grey bars: tadalafil 10 mg; dark grey bars: tadalafil 20 mg
Safety
Tadalafil 10 and 20 mg was well tolerated, with similar adverse event profiles for diabetic and non-diabetic subpopulations (Table 5). The most common treatment-emergent adverse events across the twelve studies were headache, dyspepsia, back pain, myalgia, and nasopharyngitis. Less than 4% of patients in any group discontinued the treatment due to adverse events. For patients receiving tadalafil 20 mg, 3.7% of patients with diabetes and 3.2% of patients without diabetes discontinued due to an adverse event, compared with 2.0% and 1.0% in the respective placebo groups. The incidence of serious adverse events was similar between tadalafil and placebo treatment groups, occurring in 5 of 201 (2.5%), 2 of 141 (1.4%), and 5 of 295 (1.7%) of patients with diabetes in the placebo, tadalafil 10 mg, and tadalafil 20 mg groups respectively. There was no increase in serious events of myocardial infarction or myocardial ischaemia with tadalafil treatment. There were no notable changes in clinical laboratory values, ECG parameters, physical examination findings, or vital signs with tadalafil treatment in patients either with or without diabetes.
Discussion
Men with diabetes mellitus are at increased risk of developing erectile dysfunction due to a number of factors, including autonomic neuropathy, vascular insufficiency, poor glycaemic control, hyperlipidaemia, and hypertension [20]. The large, well-defined patient population included in the current analysis was recruited from investigative sites in 20 countries. In this population, diabetic patients with erectile dysfunction had lower mean baseline IIEF erectile function scores, a greater likelihood of having severe erectile dysfunction, and lower self-reported success rates for vaginal penetration and intercourse completion at baseline, compared with non-diabetic patients with erectile dysfunction. These findings provide convincing support for the widely held assumption that erectile dysfunction associated with diabetes is more severe than erectile dysfunction observed in the general population. In addition, the current analyses indicate that PDE5 inhibition is efficacious for the treatment of erectile dysfunction in men with diabetes, albeit with a slightly lower response than in men without diabetes.
Previous epidemiological studies have established increased age, hypertension, hyperlipidaemia, diabetes, depression, and autonomic neuropathy as causative risk factors for erectile dysfunction. In this study the mean age of the diabetic and non-diabetic population was similar and fewer patients with diabetes were older than age 65. Therefore age did not contribute to the increased severity of baseline erectile dysfunction noted in the patients with diabetes. Hypertension, hyperlipidaemia and coronary artery disease were more common in patients with diabetes and probably contributed to the greater severity of erectile dysfunction observed in this population. Each of these comorbid conditions is associated with endothelial dysfunction, a common mechanistic link between erectile dysfunction and cardiovascular disease [21]. Endothelial dysfunction is frequently observed in patients with diabetes and has been associated with insulin resistance [22]. In our study we did not collect data to determine the proportion of patients with the metabolic syndrome, a condition that is likely to be associated with insulin resistance. Nevertheless, there was a high prevalence of pre-existing hypertension and hyperlipidaemia, which may indicate an underlying insulin resistance. Furthermore, endothelial function is impaired in the presence of hyperglycaemia, primarily through a decrease in NO bioavailability and responsiveness [23]. In addition, hyperglycaemia may produce reactive oxygen species, cause apoptosis of the nitrergic nerves, or produce smooth muscle fibrosis, further damaging the NO-cGMP erectile function pathway [24, 25].
Men with erectile dysfunction and diabetes taking tadalafil had a significant and clinically meaningful improvement in erectile function compared with placebo treatment, a finding which is consistent with the previously published study of tadalafil exclusively enrolling diabetic patients with erectile dysfunction [26]. The more severe erectile dysfunction at baseline observed in men with diabetes, and the slightly smaller improvement in erectile dysfunction, resulted in lower post-baseline intercourse success rates (53% vs 71% in patients without diabetes). Consistent with these results, 75% of diabetic patients treated with tadalafil 20 mg reported improved erections compared to 86% of patients without diabetes.
Published reports for sildenafil citrate and vardenafil also recorded significant improvements in erectile dysfunction in patients with erectile dysfunction associated with diabetes [27, 28, 29, 30]; however, endpoint success with all three medications was consistently less than the endpoint efficacy reported when the respective PDE5 inhibitor was administered to non-diabetic patients with erectile dysfunction [9, 10, 11]. Definitive conclusions on the relative efficacy of tadalafil, vardenafil and sildenafil citrate when administered to patients with erectile dysfunction and diabetes must be deferred until blinded, head-to-head comparison trials have been completed.
Tadalafil treatment improved erectile function in men with diabetes regardless of whether they had good or poor glycaemic control, and independently of whether they were taking insulin, oral medication or were managed by diet alone. Poor glycaemic control, as assessed by HbA1c levels, was previously found to be associated with more severe erectile dysfunction in 78 men with type 2 diabetes [31]. The current integrated analysis of 637 men with erectile dysfunction and diabetes further confirms the observation that inadequate glycaemic control is linked to severity of erectile dysfunction. While the treatment effect of tadalafil was similar at all levels of glycaemic control, patients with good baseline glycaemic control had better endpoint absolute intercourse success rates—the most important outcome to patient and partner. Euglycaemia could contribute to improved endothelial function, improved NO bioavailability, and enhanced favourable response to PDE5 inhibition. Because covariant factors associated with poor glycaemic control may ultimately contribute to the worsening of erectile dysfunction, men with diabetes might be better motivated to improve diabetic control, if they understood that erectile dysfunction and diabetic control are related. Further studies are needed to assess not only the effect of lower blood glucose on erectile dysfunction, but also the impact of good control on PDE5 responsiveness.
Because many of the placebo-controlled trials analysed in this report excluded patients with a previous history of inadequate response to sildenafil, it is possible that this exclusion criterion contributed to the favourable results reported for tadalafil. However, the observation that sildenafil-naïve patients recorded a similarly robust effect of tadalafil treatment to patients with a previous history of sildenafil use (and presumably favourable response) makes this unlikely.
Tadalafil, which has a terminal half-life of 17.5 hours, improves erectile function for up to 36 hours when administered to patients with erectile dysfunction of mixed aetiology [32]. In diabetic men treated with tadalafil, evidence of sustained efficacy for up to 36 hours was again observed, extending this observation to a difficult-to-treat population with a high incidence of severe erectile dysfunction.
The adverse event profile observed in patients with diabetes was similar to that in patients without diabetes, with no events unique to the diabetic population identified. Adverse events seldom resulted in discontinuation of treatment in patients either with or without diabetes. The absence of more frequent serious events of myocardial ischaemia in diabetic patients treated with tadalafil suggests that PDE5 inhibition is safe with regard to cardiovascular events.
This large integrated analysis provides convincing evidence that erectile dysfunction associated with diabetes mellitus is more severe than erectile dysfunction in men without diabetes. Tadalafil taken as needed prior to sexual activity was well tolerated and significantly improved erectile function in men with diabetes for up to 36 hours after dosing, despite the severity of erectile dysfunction in this population. The improvement was not affected by the level of baseline diabetic control or by the specific diabetic therapy received. Further investigation is needed to study the impact of tight glycaemic control on erectile dysfunction.
Abbreviations
- ANCOVA:
-
analysis of covariance
- cGMP:
-
cyclic guanosine 3′, 5′-monophosphate
- GAQ:
-
Global assessment questions
- IIEF:
-
International Index of Erectile Function
- NO:
-
nitric oxide
- PDE5:
-
phosphodiesterase type 5
- SEP:
-
Sexual Encounter Profile
References
Feldman HA, Goldstein I, Gatzichristou DG, Krane RJ, McKinlay JB (1994) Impotence and its medical and psychosocial correlates: results of the Massachusetts male aging study. J Urol 151:54–61
Martin-Morales A, Sanchez-Cruz JJ, Saenz de Tejada I, Rodriguez-Vela L, Jimenez-Cruz JF, Burgos-Rodriguez R (2001) Prevalence and independent risk factors for erectile dysfunction in Spain: results of the Epidemiologia de la Disfuncion Erectil Masculina Study. J Urol 166:569–574
Braun M, Wassmer G, Klotz T, Reifenrath B, Mathers M, Engelmann U (2000) Epidemiology of erectile dysfunction: results of the ‘Cologne Male Survey’. Int J Impot Res 12:305–311
Penson D, Latini D, Lubeck D, Wallace K, Henning J, Lue T (2003) Do impotent men with diabetes have more severe erectile dysfunction and worse quality of life than the general population of impotent patients? Results from the Exploratory Comprehensive Evaluation of Erectile Dysfunction (ExCEED) database. Diabetes Care 26:1093–1099
Knispel HH, Goessl C, Beckmann R (1992) Nitric oxide mediates relaxation in rabbit and human corpus cavernosum smooth muscle. Urol Res 20:253–257
Davidoff MS, Middendorff R, Mayer B, deVente J, Koesling D, Holstein AF (1997) Nitric oxide/cGMP pathway components in the Leydig cells of the human testis. Cell Tissue Res 287:161–170
Boolell M, Allen MJ, Ballard SA et al. (1996) Sildenafil: an orally active type 5 cyclic GMP-specific phosphodiesterase inhibitor for the treatment of penile erectile dysfunction. Int J Impot Res 8:47–52
Rajfer J, Aronson WJ, Bush PA, Dorey FJ, Ignarro LJ (1992) Nitric oxide as a mediator of relaxation of the corpus cavernosum in response to nonadrenergic, noncholinergic neurotransmission. N Engl J Med 326:90–94
Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, Wicker PA (1998) Oral sildenafil in the treatment of erectile dysfunction. N Engl J Med 338:1397–1404
Brock GB, McMahon CG, Chen KK et al. (2002) Efficacy and safety of tadalafil for the treatment of erectile dysfunction: results of integrated analyses. J Urol 168:1332–1336
Hellstrom WJ, Gittelman M, Karlin G et al. (2002) Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl 23:763–771
Noyman I, Marikovsky M, Sasson S et al. (2002) Hyperglycemia reduces nitric oxide synthase and glycogen synthase activity in endothelial cells. Nitric Oxide 7:187–193
Booth G, Stalker T, Lefer A, Scalia R (2001) Elevated ambient glucose induces acute inflammatory events in the microvasculature: effects of insulin. Am J Physiol Endocrinol Metab 280:E848–E856
Graier WF, Posch K, Fleischhacker E, Wascher TC, Kostner GM (1999) Increased superoxide anion formation in endothelial cells during hyperglycemia: an adaptive response or initial step of vascular dysfunction? Diabetes Res Clin Pract 45:153–160
Fonseca V, Desouza C, Asnani S, Jialal I (2004) Nontraditional risk factors for cardiovascular disease in diabetes. Endocrine Reviews 25:153–175
Desouza C, Akers D, Parulkar A, Fonseca VA, Lumpkin D (2002) Acute and prolonged effects of sildenafil on brachial artery flow-mediated dilatation in type 2 diabetes. Diabetes Care 25:1336–1339
Calles-Escandon J, Cipolla M (2001) Diabetes and endothelial dysfunction: a clinical perspective. Endocr Rev 22:36–52
Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A (1997) The International Index of Erectile Function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 49:822–830
Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH (1999) Diagnostic evaluation of the Erectile Function Domain of the International Index of Erectile Function. Urology 54:346–351
Vinik A, Richardson D (1998) Erectile dysfunction in diabetes. Diabetes Rev 6:16–33
Kaiser DR, Billups K, Mason C, Wetterling R, Lundberg JL, Bank AJ (2004) Impaired brachial artery endothelium-dependent and -independent vasodilation in men with erectile dysfunction and no other clinical cardiovascular disease. J Am Coll Cardiol 43:179–184
Williams SB, Goldfine AB, Timimi FK et al. (1998) Acute hyperglycemia attenuates endothelium-dependent vasodilation in humans in vivo. Circulation 97:1695–1701
Williams SB, Cusco JA, Roddy MA, Johnstone MT, Creager MA (1996) Impaired nitric oxide-mediated vasodilation in patients with non-insulin-dependent diabetes mellitus. J Am Coll Cardiol 27:567–574
Cellek S, Foxwell NA, Moncada S (2003) Two phases of nitrergic neuropathy in streptozotocin-induced diabetic rats. Diabetes 52:2353–2362
Cellek S, Qu W, Schmidt AM, Moncada S (2003) Synergistic action of advanced glycation end products and endogenous nitric oxide leads to neuronal apoptosis in vitro: a new insight into selective nitrergic neuropathy in diabetes. Diabetologia 47:331–339
Saenz De Tejada I, Anglin G, Knight JR, Emmick JT (2002) Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care 25:2159–2164
Goldstein I, Young JM, Fischer J, Bangerter K, Segerson T, Taylor T (2003) Vardenafil, a new phosphodiesterase type 5 inhibitor, in the treatment of erectile dysfunction in men with diabetes: a multicenter double-blind placebo-controlled fixed-dose study. Diabetes Care 26:777–783
Price DE, Gingell JC, Gepi-Attee S, Wareham K, Yates P, Boolell M (1998) Sildenafil: study of a novel oral treatment for erectile dysfunction in diabetic men. Diabet Med 15:821–825
Rendell MS, Rajfer J, Wicker PA, Smith MD (1999) Sildenafil for treatment of erectile dysfunction in men with diabetes. JAMA 281:421–426
Stuckey BG, Jadzinsky MN, Murphy LJ et al. (2003) Sildenafil citrate for treatment of erectile dysfunction in men with type 1 diabetes: results of a randomized controlled trial. Diabetes Care 26:279–284
Romeo JH, Seftel AD, Madhun ZT, Aron DC (2000) Sexual function in men with diabetes type 2: association with glycemic control. J Urol 163:788–791
Porst H, Padma-Nathan H, Giuliano F, Anglin G, Varanese L, Rosen R (2003) Efficacy of tadalafil for the treatment of erectile dysfunction at 24 and 36 hours after dosing: a randomized controlled trial. Urology 62:121–125
Acknowledgements
Diabetes Research at Tulane University is supported in part by the Tullis Tulane Alumni Chair in Diabetes and the Susan Harling Robinson Fellowship in Diabetes Research. The authors acknowledge Linda MacKeen (ICOS Corporation, Bothell, Washington, USA) for medical writing assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of interest statement: Funding for the studies and these analyses was provided by Lilly ICOS LLC. Drs Fonseca and Seftel did not receive any compensation from the sponsor for this analysis and the writing of this paper. Dr Fonseca does not have any conflicts of interest to declare. Dr Seftel is a consultant to Auxilium, Bayer, ICOS, LillyICOS LLC and Pfizer.
Rights and permissions
About this article
Cite this article
Fonseca, V., Seftel, A., Denne, J. et al. Impact of diabetes mellitus on the severity of erectile dysfunction and response to treatment: analysis of data from tadalafil clinical trials. Diabetologia 47, 1914–1923 (2004). https://doi.org/10.1007/s00125-004-1549-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1549-6