
Abstract
At least 17 million people die from acute myocardial infarction (AMI) every year, ranking it first among causes of death of human beings, and its incidence is gradually increasing. Typical characteristics of AMI include acute onset and poor prognosis. At present, there is no satisfactory treatment, but development of coronary collateral circulation (CCC) can be key to improving prognosis. Recent research indicates that the levels of cytokines, including those related to promoting inflammatory responses and angiogenesis, increase after the onset of AMI. In the early phase of AMI, cytokines play a vital role in inducing development of collateral circulation. However, when myocardial infarction is decompensated, cytokine secretion increases greatly, which may induce a cytokine storm and worsen prognosis. Cytokines can regulate the activation of a variety of signal pathways and form a complex network, which may promote or inhibit the establishment of collateral circulation. We searched for published articles in PubMed and Google Scholar, employing the keyword “acute myocardial infarction”, “coronary collateral circulation” and “cytokine storm”, to clarify the relationship between AMI and a cytokine storm, and how a cytokine storm affects the growth of collateral circulation after AMI, so as to explore treatment methods based on cytokine agents or inhibitors used to improve prognosis of AMI.
Similar content being viewed by others


Introduction
According to global statistics, the death toll of ischemic heart disease (IHD) in 2019 increased by 2 million to 8.9 million, accounting for 16% of total deaths, making it the number one killer worldwide [1]. The European Society of Cardiology (ESC) recently released a set of statistics related to IHD in 2019. It was estimated that there were 5.8 million new cases and 47.6 million patients in its 57 member countries [2]. Moreover, ST-segment elevation myocardial infarction (STEMI) is becoming increasingly prevalent with an annual incidence of about 40–140 per 10000 [3]. In most developed countries, coronary atherosclerosis continues to be one of the leading causes of mortality in patients who develop coronary artery disease [4]. Similarly, the rapidly growing rate of acute myocardial infarction (AMI) in China has drawn public attention. Some experts predict that by 2030, the annual number of patients with AMI in China may exceed 23 million because of increased urbanization and behavioral risks [5]. Not only will primary AMI put lives at risk but recurrent AMI must also be considered. The latest China PEACE prospective AMI study indicated that the 1-year mortality rate of patients with recurrent AMI was 25 times higher than that for primary AMI. Furthermore, early after discharge—meaning within the first 30 days—more than one-third of patients suffered from recurrent AMI [6]. The later that patients receive emergency care after onset of AMI, the worse the outcome may be, and while the median time from the onset of symptoms to reaching the hospital is only 2–3 h in the United States and other western countries, it is 4 h in China [7]. Moreover, especially in the past 3 years, it has become apparent that coronavirus disease 2019 (COVID-19) can attack the human cardiovascular system, which can manifest as AMI, resulting in an increase in cardiac biomarkers [8, 9]. All the above factors contribute to the harm done by AMI to human health all over the world. Therefore, it is important to explore methods of treatment beyond those that currently exist.
We had noticed that after the occurrence of AMI, clinical outcomes in some patients seemed to be associated with differences in formation of CCC. Moreover, patients who had more collateral circulation had less myocardial necrosis than those with incomplete collateral circulation. Studies have also shown that development of CCC can maintain perfusion of infarcted myocardium to prevent fatal acute myocardial ischemia–reperfusion injury (IRI). In addition, collateral angiogenesis is of great importance for myocardial healing and remodeling after AMI, although it develops too slowly to provide for acute myocardial protection [10]. Thus, the development of collateral circulation may not only reduce mortality of AMI events but may also reduce recurrent AMI. Additionally, laboratory tests have shown that AMI patients exhibit leukocytosis and release of various angiogenic and inflammatory factors, suggesting that they are related to a systemic inflammatory response [11]. Nevertheless, there are few reports on the correlation between increased cytokine levels and collateral angiogenesis, and it is worth noting that they share some regulatory factors and signaling pathways. We take this as a starting point to put forward a new hypothesis: a brief cytokine storm occurs after AMI and it impacts collateral angiogenesis. At the same time, due to different levels of cytokines and inherent collateral vessels, the cytokine storm may lead to heterogeneity in CCC. This paper elaborates on this hypothesis and explores the mechanism and interactions between the cytokine storm and formation of CCC following AMI. Our intention is to propose a new direction for the study of CCC and provide ideas for exploring new treatments for AMI.
We searched for published articles in PubMed and Google Scholar, employing the keyword “acute myocardial infarction” and “prognosis”, and found that positive CCC can effectively improve the prognosis of AMI. After searching for "cytokine storm", “cytokine release syndrome” and “acute myocardial infarction”, it was found that AMI induces cytokine production and activation to a certain extent. Through further reading, we found that cytokine storm and AMI can interact as both cause and effect. Through the connection with the above, we concluded our own conjecture that cytokine storm affects the prognosis of AMI by affecting the generation of CCC. We further identified seven key cytokines and their effects on coronary collateral angiogenesis. We conclude how cytokine storm leading to heterogeneity in CCC after AMI. Finally, we searched for inhibitors of relevant cytokines or pathways and activators of pro-angiogenic factors to explore effective treatment of AMI.
Coronary collateral circulation
Coronary collateral circulation refers to a network of cardiac vascular anastomoses that often develop after coronary artery stenosis or secondary thrombosis caused by coronary atherosclerosis. Collateral vessels are highly dilated with thin walls, which are at risk of rupture and bleeding in the presence of inflammatory factors. Common pathways of collateral circulation include anterior and posterior descending branches, anterior and posterior septal branches, diagonal branches and obtuse marginal branches, among others.
As is well known, collateral circulation is innate and well-developed in humans. During embryogenesis, endothelial progenitor cells derived from mesoderm form the first blood vessels through continuous proliferation and differentiation. Functional collateral vessels begin to develop during the neonatal period, while bone marrow-derived endothelial progenitor cells enter the blood circulation and accumulate at sites of angiogenesis in adults [12]. Additionally, the formation of CCC is divided into early opening and late formation [13]. Angiography has demonstrated formation of collateral vessels on the 10th day after persistent acute occlusion, and further functional maturation occurs by the 12th week [14]. Cardiac autopsy of 1050 adult patients showed that 46% of the hearts had structural anastomosis among coronaries. Specifically, the incidence of coronary artery anastomosis was 9% in normal hearts, 63% in patients with marked arterial stenosis, and 95% in those with chronic total coronary occlusion [15]. It is therefore apparent that in the case of arterial stenosis in the human heart, compensatory collateral anastomosis often occurs to improve blood and oxygen supply.
Research on the mechanism by which collateral microcirculation is generated has been relatively extensive. After acute ischemia and hypoxia in cardiomyocytes, collateral circulation is mainly generated through angiogenesis and vascular remodeling [16]. Angiogenesis requires the participation of a variety of cells, among which pericytes are indispensable to the generation and evolvement of new capillaries. In addition, maturation of larger blood vessels undoubtedly requires participation of smooth muscle cells. Neovascularization originates in pre-existing blood vessels and develops from inherent nerve plexuses through germination and intussusception. Germination refers to the gradual lengthening of micro-vessels and reformation of the vascular lumen. At first, endothelial cells (ECs) in pre-existing capillaries are activated and the basement membrane is degraded. Subsequently, ECs migrate to the surrounding stroma and align with each other to extend micro-vessels and reshape the lumen. Intussusception refers to reorganization of ECs in capillaries at junctions. Pericytes and myo-fibroblasts grow into the invaginated lumen and release collagen fibers that contribute to lumen enlargement and splitting into two new capillaries. By contrast, vascular remodeling does not occur by regeneration, but by opening, thickening and twisting of the anastomoses between coronary arteries. One previous study showed that positive remodeling of arterioles can form arteries 12 times larger than their original size [16]. Furthermore, a micro-vessel can form a branch between the proximal and distal ends of the same occluded coronary artery. Therefore, the blood supply to the ischemic area can be restored through such self-bypass mechanisms.
Because cardiac ischemia and hypoxia can lead to several serious adverse outcomes, development of collateral circulation has a significant impact on disease prevention and prognosis. During transient vascular occlusion, a quarter of myocardial ischemic events in people who did not have underlying coronary artery disease could be prevented by preformed collateral arteries. When AMI occurs, well-developed collateral circulation can reduce the size of the infarct and improve the prognosis of the patient. CCC supplies blood to the myocardial tissue surrounding the occluded blood vessels, preventing myocardial necrosis and formation of ventricular aneurysms that result from prolonged ischemia and hypoxia. In chronic total coronary occlusion lesions, collateral branches provide on average 39% of the blood flow that occurs in unobstructed coronary arteries [17]. Research has confirmed that lower heart failure risk is strongly associated with formation of collateral vessels in areas of infarct-related arteries after myocardial infarction (MI). Although increased collateral circulation reduces long-term mortality, it does not influence the risk index for re-infarction [18]. However, several studies have shown that CCC increases mortality and is a risk factor for ischemic revascularization after percutaneous coronary intervention (PCI) [19].
Interestingly, studies have reported differences in the formation of collateral vessels after AMI. Specifically, epicardial collaterals are more likely to form than medial collaterals [14, 20]. During early formation of collateral arteries, the left coronary branches span the watershed to connect with right coronary branches. The ligated branches are also observed to anastomose with non-ligated branches of the left coronary artery through its most distal branches [20]. However, few studies have investigated whether new collateral circulation in different parts of the heart exhibits different volume, shape and function. Further research in this area will help to fill gaps in the understanding of collateral artery formation.
Development of collateral circulation is a complicated process involving various factors in the in vivo environment, including physical fluid shear stress (FSS), cytokines, such as TNF-α, IL-6, TGF-β, vascular cell adhesion molecule-1 (VCAM-1), vascular endothelial cell growth factor (VEGF), monocyte chemoattractant protein-1 (MCP-1) and pigment epithelium-derived factor (PEDF), among others. Moreover, formation of vessels also depends on signaling pathways, such as NF-κB, JAK/STAT and PI3K, and gene expression such as that of transcription factor DACH1, which regulates the CXCL12/CXCR4 signaling axis, and transcription factor NFAT5, which induces MCP-1 secretion, in addition to other factors such as systemic hypoxemia.
In the following sections, we explore the roles of various cytokines and signaling pathways related to angiogenesis, which along with various cell types, form a complex regulatory network that cannot be simply explained by any single factor that controls its mechanism. Subsequently, we discuss how cytokines influence the development of collateral circulation.
Cytokine storm after myocardial infarction
Cytokine storm and myocardial infarction: mutual cause and effect
A cytokine storm originates from a systemic inflammatory response that is difficult to control. It is triggered by multiple factors and characterized by the production of pro-inflammatory cytokines or chemokines and results in insufficiency of multiple organs. An uncontrolled cytokine storm is particularly damaging to the heart. Additionally, the continuous accumulation and enhancement of a cytokine storm in the heart can cause myocarditis, arrhythmia, and in severe cases, myocardial ischemia and infarction. Numerous studies have focused on how a cytokine storm is formed and how it leads to MI. However, there are few studies on the mechanisms of cytokine action on collateral circulation. Studies of venous blood from MI patients have revealed significantly increased levels of cytokines, especially IL-6, TNF-α, and MCP-1 [11, 21, 22]. More in-depth studies found different levels of cytokine expression after MI, as well as different levels of coronary collateral growth [22, 23]. Currently, most of these inflammatory factors are only used for diagnostic evaluation of MI. We speculate that some level of cytokine storm is induced after MI, and that these cytokines have an important impact on subsequent collateral growth. That is to say that knowledge of the levels and proportions of these cytokines can form the basis of prognostic assessment and treatment of MI [24].
The emergence of a cytokine storm after myocardial infarction
The emergence and intensification of a cytokine storm after MI can be affected by many factors. Cytokines stimulate production of other cytokines, all of which trigger a storm and synergistically damage myocardium. During MI, cardiomyocytes undergo autophagy and programmed apoptosis, of which inflammatory factors are key regulators [25]. Early-induced inflammatory factors and immune cells take part in protecting tissues. They mainly induce proliferation of fibroblasts and other cell types, thereby promoting myocardial structural remodeling and functional recovery, allowing inflammation to quickly subside [26, 27]. After the onset of the inflammatory response, in most cases the body's compensatory repair mechanisms fully restore normal function to tissues and organs. However, persistent cytokines are associated with late cardiac contractility and poor prognosis [25]. If the heart is infected by pathogens, infarction will lead to the release of more pathogens, which can over-stimulate the immune system and cause immune dysfunction.
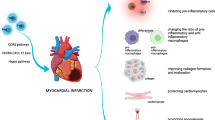
Both innate and acquired immunity play fundamental roles in the activation of a cytokine storm. Cytokine levels do not continue to decline after MI, and innate immunity activates adaptive immune cells like T cells to release pro-inflammatory cytokines and chemokines that further activate innate immune cells, such as macrophages, dendritic cells and ECs. Activated cells release more cytokines through autocrine or paracrine mechanisms, which further stimulate activation of more immune cells and ECs. If excessive inflammatory cytokines and chemokines accumulate in the heart, a large-scale inflammatory cascade can result that leads to cardiac insufficiency, which seriously affects cardiac prognosis [28]. It is worth noting that not all cytokines released after AMI inhibit formation of CCC in the heart, and some can also promote it (Fig. 1) [29]. We classified these cytokines as cardio-protective or cardio-damaging. Protective cytokines include VEGF, MCP-1, and TGF-β, while damaging cytokines include IL-1, IL-6, and TNF-α [30]. Different proportions and levels of cytokines in diverse patients with MI promote growth of collateral circulation and ultimately lead to a specific prognosis of cardiac function.

Mechanisms of the effects of a cytokine storm on the heart following myocardial infarction. A CXCL12 and TNF-α promote proliferation and activation of vascular smooth muscle cells (VSMCs) to maintain collateral vessel integrity. B TGF-β, MCP-1, TNF-α and G-CSF activate fibroblasts, increase collagenous fiber secretion to promote cardiac remodeling, and induce branching of collateral circulation. C VEGF promotes formation of new blood vessels. D Excessive TNF-α and IL-1 can directly induce apoptosis and necrosis of hypoxic cardiomyocytes
Key cytokines
After MI, cytokines are activated in cascades, and key cytokines increase accordingly, including pro-inflammatory factors, such as IFN-γ, TNF-α, IL-1, IL-6, IL-10 and IL-18, and angiogenesis-promoting factors, such as VEGF and PDEF. The levels of the IFN-γ-induced chemokines CXCL9 and CXCL10 also increase significantly [24]. In addition, several signaling pathways are involved, including the NF-κB, JAK/STAT and PI3K pathways [29]. Cytokines and signaling pathways interweave and interact with each other to form a closely interconnected cytokine signaling network, which has a crucial impact on collateral circulation after MI. In the following sections, attention will be focused on IL-1, IL-6, IL-12, TNF-α, VEGF, MCP-1 and TGF-β, their interactions with other cytokines, and effects on the cardiovascular system (Fig. 2).

Signaling pathways in response to binding of cytokines to receptors. A IL-1α and IL-1β combine with IL-1 receptor (IL-1R) to up-regulate the activity of caspase-1 and caspase-9; B TNF-α combines with TNF receptor (TNFR) to activate caspase-3, caspase-8 and caspase-9, and activate the NF-κB and JAK/STAT signaling pathways; C IL-6 combines with IL-6 receptor (IL-6R) to activate the JAK/STAT signaling pathway; D IL-12 combines with IL-12 receptor (IL-12R) to activate the JAK/STAT signaling pathway; E VEGF combines with VEGFR2 to activate the PI3K/Akt signaling pathway; F TGF-β combines with TGFBR1/ALK5 receptor to inhibit activation of endothelial cells (ECs) by the Smad2/3 cascade; TGF-β combines with ACVRL1/ALK1 receptor to stimulate proliferation of ECs by the Smad1/5 cascade; G MCP-1/CCL2 combines with high affinity C–C chemokine receptor type 2 (CCR2) to induce monocyte macrophage recruitment
IL-1
Interleukin (IL)-1 is capable of activating the fibrotic pathway and promoting cardiomyocyte apoptosis, leading to an aseptic inflammatory response [31]. Therefore, IL-1 plays an essential role in the inflammatory response to MI. Furthermore, IL-1 induces cardiomyocyte apoptosis by upregulating the activities of caspase-1 and caspase-9. It is worth noting that IL-1α and IL-1β play significant roles in the occurrence and progression of MI. IL-1α is mediated by the IL-1 receptor (IL-1R), which is able to attract monocytes and neutrophils to the site of vascular injury and to evoke inflammatory responses. In addition, IL-1α promotes expression of VCAM-1 on ECs so as to increase leukocyte-endothelial cell adhesion in the circulation [32]. Furthermore, many pro-inflammatory factors are released after MI. IL-1β is activated early, and then IL-6, TNF-α and other cytokines are successively activated [33]. Arguably, IL-1β can be considered to be the promoter of multiple signaling cascades [34]. It has been suggested that IL-1β has an adverse effect on the growth of bone marrow colonies, but the intravascular function of bone marrow can be restored by blocking the IL-1 receptor (IL-1R) [30]. Administration of recombinant IL-1R antagonist immediately or 24 h after ischemic attack can significantly reduce cardiomyocyte apoptosis. It has been shown that if IL-1 activity is not minimized, it inhibits myocardial healing and can even lead to cardiac rupture [34].
IL-6
Multiple signaling cascades in cells can be activated by IL-6 binding to its receptor complex (IL-6R). The most representative pathway is the JAK/STAT pathway, with JAK1 being the most critical Janus kinase (JAK). Signal transmission involving JAK1 can be activated by IL and IFN. After JAK1 phosphorylation, intracellular tyrosine residues begin to recruit STAT molecules, which are then phosphorylated by JAKs. Subsequently, the gene is translated and transcription is activated [35]. There are three pathways for activation of JAK/STAT signaling by IL-6: classical signaling, trans-signaling and trans-presentation [36]. The classical pathway mainly plays a role in anti-inflammatory signaling, while the others act in opposite ways. In the presence of excessive IL-6 secretion, the pro-inflammatory effect is stronger than the anti-inflammatory effect, which often results in a waterfall inflammatory response [37]. It has been shown that IL-6, granulocyte colony stimulating factor (G-CSF), hypoxia and inflammation are rapidly up-regulated in the first 24 h after MI. When the JAK/STAT pathway is activated, other signal proteins are also up-regulated, including PI3K, Akt, p38 MAPK, ERK, NF-κB and nitric oxide synthase (NOS). These downstream signals mainly promote cell proliferation and migration. The JAK/STAT pathway is further activated after an increase in activity of these signaling pathways [38]. Moreover, while different types of STAT are activated, their effects are distinct and balance each other's activities. STAT1 can induce apoptosis-promoting molecules, such as caspase-1, Fas and FasL, resulting in cardiomyocyte apoptosis and myocardial injury. In fibroblasts and cardiomyocytes, STAT3 activation acts to resist the pro-apoptotic effect of STAT1. Additionally, it protects cardiomyocytes not only through upregulation of Bcl-2 but also reduction of Bax and caspase-331 [39]. After AMI, both myocardial hypertrophy and cardiac remodeling can result from activation of the JAK/STAT signaling pathway [40]. Activation of STAT3 and STAT5 can also stimulate reactive oxygen species (ROS) pathways, induce upregulation of the transcription factor HIF-1, and promote VEGF secretion and VEGFR expression. ROS can activate protein kinases and promote angiogenesis in a hindlimb ischemia model. Although physiological ROS production can activate the JAK/STAT pathway, excessive ROS production has the opposite effect [41].
IL-12
IL-12 is mainly produced by CD11b + monocytes and it can aid the growth of mature Th1 effector cells, which are differentiated from naive CD4 + T cells, to promote IFN-γ8 secretion. Studies have shown that inhibition of angiogenesis by IL-12 depends on monocytes. During AMI and hindlimb ischemia, IL-12 knockout mice exhibited increased angiogenesis, which implies that inhibition of IL-12 can protect cardiac function by promoting angiogenesis and reducing inflammation [42]. Signal transduction is mainly mediated by the JAK-STAT family. The combination of IL-12 with its receptor (IL-12R) can lead to activation of STAT1, STAT3 and STAT4 [43]. After measuring the levels of plasma inflammatory markers in patients with and without cardiovascular events, it was found that IL-12 increased in patients with unstable angina pectoris, AMI and death [44].
TNF-α
Tumor necrosis factor (TNF)-α promotes mitosis of vascular smooth muscle cells (VSMCs) in human arteries by activating the NF-κB signaling pathway, which participates in induction of angiogenesis and ventricular remodeling [45, 46]. Recent studies have confirmed that the concentration of TNF-α in infarcted and non-infarcted myocardium increases after MI, which means that TNF-α is not only enriched in and around the infarcted region but also up-regulated in the contralateral normal region of myocardium [40, 46]. Therefore, it should be noted that patients with continuously elevated TNF-α levels are also at greater risk of recurrent and multiple coronary events [47]. Furthermore, TNF-α can stimulate ECs and leukocytes to produce pro-inflammatory cytokines, chemokines and adhesion molecules through the NF-κB signaling pathway, enhancing the local inflammatory response [48, 49]. NF-κB is considered to be a typical pro-inflammatory signaling pathway [50], and its activation launches a genetic program leading to expression and activation of cytokines, chemokines and matrix metalloproteinases (MMPs). In addition, it promotes inflammation and fibrosis, which are involved in myocardial remodeling [51].
TNF-α can stimulate apoptosis by activating caspase and activator protein-1 (AP-1), and by cooperating with other cytokines such as IFN-γ [52,53,54,55]. The caspase pathway activates TNF receptor (TNFR)-related death domain (TRADD) and Fas-related death domain (FADD) proteins. Finally, caspase-3, caspase-8 and caspase-9 are activated to induce apoptosis. Caspase can also be activated by the release of ROS from mitochondria, while AP-1 can be activated by extracellular-signal-regulated kinase (ERK), p38 mitogen-activated protein kinase (p38MAPK) and c-Jun N-terminal kinase (JNK) [56]. Thus, TNF-α can bring about a series of changes through activation of downstream pathways. In addition, not only can it change the extracellular matrix of myocardium and promote fibrous tissue formation, but TNF-α can destroy collagen fibers in myocardium and cause denaturation. In severe cases, it induces cardiomyocyte apoptosis and causes irreversible myocardial injury. It is worth mentioning that JAK/STAT signaling is of great importance for signal transduction in response to TNF-α. Therefore, cardiomyocyte hypertrophy can result from activation of JAK/STAT signaling and STAT overexpression after MI [29, 40]. Moreover, JAK/STAT may also affect the NF-κB pathway, leading to activation of other cytokines, such as IL-6 and IL-17, to further induce MI [40, 57]. In sum, the strong pro-inflammatory effect of TNF-α, which may cause great damage to the body, cannot be ignored even though it can stimulate formation of VSMCs. The superposition of these two processes makes the net effect of TNF-α more complex. Further in-depth research will deepen our understanding of this important cytokine and provide innovative ideas for new treatment schemes.
VEGF
The vascular endothelial growth factor (VEGF) family is composed of VEGF-A, VEGF-B, VEGF-C, VEGF-D and PGF [58], with VEGF-A being the most potent. It can be secreted by multiple cells in vascular tissue, such as vascular endothelial cells, fibroblasts, smooth muscle cells and immune cells, all of which contribute to angiogenesis by having vascular endothelial growth factor receptors (VEGFRs) on their surfaces. VEGFR mainly exists on the surface of vascular endothelial cells in the form of VEGFR1 (F1t-1) and VEGFR2 (KDR/Flk-1). VEGFR2 is much stronger than VEGFR1 in promoting survival, proliferation and migration of ECs in the process of VEGF-induced angiogenesis [59]. After the VEGF/VEGFR2 signaling pathway is activated, VEGFR2 starts to activate multiple downstream signaling pathways, including the phosphatidylinositol 3-kinase (PI3K)/Akt pathway that inhibits apoptosis, the p38 MAPK and focal adhesion kinase (FAK) pathways that mediate cell migration, the RAS/Raf/MEK/MAPK and PLCγ/IP3 pathways that mediate signal transcription and enhance cell migration and proliferation, and the PLCγ and Akt/PKB pathways that regulate vascular permeability [60,61,62,63,64]. It is worth noting that the PI3K/Akt signaling pathway elicits a significant cardio-protective effect. PI3K affects growth and development of cardiomyocytes regulated by insulin and insulin-like growth factor-1 (IGF-1) in cardiomyocytes. Moreover, when endothelial nitric oxide synthase (eNOS) is activated by PI3K, a large amount of nitric oxide (NO) is produced. Activation of this pathway can antagonize ROS pathways and reduce cell apoptosis [49]. Hence, PI3K is essential for cardiac physiology and prevention of pathological heart remodeling and failure [65].
Activated VEGFR2 can also regulate signaling pathways in cells by being internalized [58]. Some studies have also shown that the reactive oxygen species-endoplasmic reticulum (ROS-ER) stress autophagy axis is likely to be involved in VEGFR2-induced angiogenesis [66]. Although VEGF-A increased significantly after MI, some patients had a reduced angiogenic response to VEGF due to a VEGFR gene mutation, which may be one of the reasons for differences between patients in the formation and prognosis of collateral circulation.
MCP-1/CCL2
Monocyte chemoattractant protein-1 (MCP-1) is also known as chemokine CC-motif ligand 2 (CCL2). Clinical analysis confirmed that MCP-1 levels are significantly higher in the serum of STEMI patients [67]. Compared with patients who had well-developed collateral circulation, patients with missing collateral circulation had substantially lower plasma MCP-1 levels [68]. Up-regulated MCP-1 mainly recruits monocytes and macrophages to atherosclerotic lesions within the infarct area by binding to high affinity CCR2 to induce infiltration of immune cells and formation of new collateral arteries that reduce infarct area and scar formation. It can also directly promote differentiation of cardiac fibroblasts into myo-fibroblasts to maintain cardiac function after MI [69]. In addition, MCP-1 may regulate gene transcription and expression, stimulate production and degradation of extracellular matrix, and cause cardiac interstitial fibrosis [48, 70, 71]. In the early phases of MI healing, MCP-1 can accelerate wound healing and in time clear the healing infarct tissue through various regulatory pathways. For example, MCP-1 can stimulate generation of TNF-α, IL-1β and IL-6, promote angiogenesis, regulate MMP activity and modify collagen expression in fibroblasts [72]. In subsequent myocardial remodeling, MCP-1 may increase inflammation and deposition of fibrous tissue, which may be detrimental to ventricular remodeling and lead to adverse clinical outcomes [70, 73].
TGF-β
Transforming growth factor (TGF)-β can be induced and activated in MI. It mainly mediates tissue fibrosis related to inflammation and tissue injury by inducing phosphorylation of Smads proteins and hence participates in regulation of cardiac repair. The Smads protein family can have dual effects on proliferation and migration of ECs. TGF-β can inhibit activation of ECs by the Smad2/3 cascade by binding to the TGFBR1/ALK5 receptor, and it can promote proliferation of ECs through the Smad1/5 cascade by binding to the ACVRL1/ALK1 receptor [74,75,76]. AMP-activated protein kinase (AMPK), located upstream of the TGF-β/Smads signaling pathway, is also involved in regulation and myocardial protection [77]. In the healing infarct, TGF-β can promote cell migration by mediating synthesis of extracellular matrix proteins and upregulation of tissue inhibitor of metalloproteinase (TIMP) through the Smad3 signaling pathway. At the same time, TGF-β significantly increases synthesis of type I and type III collagen, decreases expression of collagenase, and increases synthesis of TIMP-1. In the post infarction remodeling stage, TGF-β can induce cardiomyocyte hypertrophy by activating TAK1, and at the same time enhance TIMP synthesis in fibroblasts, resulting in dilated remodeling of infarcted ventricle [78].
Heterogeneity of collateral circulation caused by a cytokine storm
Previous studies have shown that necrotic cardiomyocytes following AMI will induce a transient cytokine storm, and that the inflammatory response and neovascularization mediated by the cytokine storm are heterogeneous, which leads to differences in CCC. In the previous section we summarized how several key cytokines are involved in collateral angiogenesis, and in this section we will describe how cytokines interact to form cytokine storms and affect collateral angiogenesis.
In the early stage of myocardial hypoxia, blockage of blood flow channels can be caused by emboli. At this time, there is an increase in shear stress resulting from blood flow along the endothelial surface, which is an important initiating factor of collateral angiogenesis [79,80,81]. (Fig. 3) The sensitivity of ECs to proliferation signals increases after mechanical stimulation, which leads to secretion of the cytokines MCP-1 and VCAM-1 to attract monocytes and lymphocytes. Immune cells continue to secrete MMPs to dissolve the matrix around blood vessels, which leads to proliferation, separation and migration of ECs to form new blood vessels [21, 82, 83]. A cytokine storm includes activation of many cytokines, but usually in a defined sequence [21]. It has been shown that VEGF and IL-6 increase significantly in the early stage of MI, with VEGF playing the most critical role in angiogenesis. It is secreted in large quantities in response to shear force, and its ability to induce EC proliferation and migration is also critically important [21]. At the eye of a cytokine storm, IL-6 plays a leading role in activation of other cytokines via many downstream pathways, with such continuous positive feedback resulting in a cascade effect. IL-6 can not only promote secretion of VEGF through the JAK/STAT pathway, but also induce protective cytokines, such as TGF-β, TNF-α, G-CSF and MCP-1 [84]. They promote differentiation of fibroblasts and early remodeling in the heart and blood vessels to maintain stable cardiac function. CXCL12/CXCR4 can not only up-regulate the levels of VEGF and VEGFR but also increase neovascularization through promotion of VSMC proliferation [85]. TNF-α can induce formation of vascular smooth muscle through the NF-κB pathway [45].

Formation of collateral circulation after coronary artery embolism. A Vascular embolization leads to hypoxia of endothelial cells (ECs) and formation of fluid shear stress (FSS). Hypoxia and FSS jointly induce ECs to produce cytokines, such as MCP-1 and VCAM-1, to attract and activate immune cells. ECs also produce MMPs and VEGF to degrade the surrounding matrix and promote their own migration and proliferation. B ECs escape from the original vascular wall and form bud-like tubular anastomoses through sustained migration and proliferation. C Vascular smooth muscle cells (VSMCs) are also activated and proliferate in response to stimulation by cytokines, and gradually surround the outer layer of new blood vessels. D Fibroblasts integrate into the walls of new blood vessels, secrete collagen fibers to form the peri-cellular matrix, and increase branching of collateral circulation
When myocardial ischemia reaches a certain level, MI results and secretion of cytokines increases greatly. Excess IL-1, TNF-α and IL-6 now act as myocardial-damaging cytokines. Early TNF-α can up-regulate intercellular adhesion molecule-1 (ICAM-1) through the NF-κB pathway and antagonize apoptosis to protect the myocardium. However, studies have found that inhibiting TNF-α after MI can improve prognosis [86]. Apart from activating the NF-κB pathway in the presence of excess TNF-α, pro-apoptotic pathways become more prominent. TNF-α can induce myocardial apoptosis mainly by activating caspase and AP-1. Furthermore, excessive IL-1β can also activate inflammatory bodies and caspase so as to induce apoptosis. IL-1β can also lead to cell swelling, rupture and apoptosis through cleavage of gasdermin-D (GSDM-D), which also results in release of more cytokines [87]. Excessive levels of cardiomyocyte damaging factors attract large numbers of immune cells. They then begin to attack ECs and stromal cells, resulting in obstruction of collateral circulation. Ultimately, MI is irreversible and may lead to the spread of lesions. Therefore, we believe that in the cytokine storm that follows MI, there are mutual constraints between protective and damaging cytokines that have an important impact on the formation of collateral circulation. It is worth noting that as a result of heterogeneity in physiology, degree of vascular stenosis, cell microenvironment and cytokine secretion among different individuals, the intensity of a cytokine storm and its positive or negative impact on collateral angiogenesis is expected to vary, which can account for differences in collateral circulation between patients.
Treatment
Development of treatments that promote collateral circulation after MI remains a major challenge in cardiovascular medicine. Therapeutic angiogenesis typically involves promotion of collateral circulation based on the existing vascular system, which has been proposed and studied by scientists for many years for treatment of a variety of conditions, including ischemic disease [88]. The current approaches to therapeutic angiogenesis include gene therapy, cell therapy, and protein therapy. However, these methods all have disadvantages in the clinical setting.
As discussed above, we suggest that a cytokine storm after MI affects formation of collateral blood vessels. Mechanistically, current therapies use three approaches: inhibition of pro-inflammatory factors, promotion of pro-angiogenic factors, and regulation of related signaling pathways (Table 1).
Inhibition of secretion of pro-inflammatory factors
As mentioned above, although early-induced inflammatory factors can protect myocardial tissue, continued secretion of pro-inflammatory cytokines will induce a cytokine storm, which is not conducive to development of collateral circulation and recovery of cardiac function. Therefore, taking appropriate steps to inhibit inflammatory factors will help to promote myocardial remodeling and cardiac function after MI. Current studies have shown that statins can play an anti-inflammatory role. For example, rosuvastatin may effectively inhibit local production of TNF-α and p38 MAPK activity by down-regulating the TNF-α/p38 MAPK signaling pathway. Therefore, it can inhibit the inflammatory response and reduce myocardial fibrosis [89, 90]. Simvastatin can reduce secretion of IL-6 and MCP-1 in ECs and reduce the damage done by inflammatory cytokines to ischemic myocardium [91,92,93]. Related treatments have also been reported, including photoluminescent mesoporous silicon nanoparticles with siCCR2, CCR2-targeting PEG-DSPE micelles that reduce monocyte recruitment, and use of the nonagonist CCL2 competitor PA508, among others [94,95,96].
In recent years, clinical studies have found that blocking IL-1 is beneficial for IHD and can also improve cardiac remodeling in patients with STEMI, among which the IL-1R antagonist anakinra has been more thoroughly studied [97]. Following anakinra treatment, the concentration of C-reactive protein (CRP) decreased, along with a significant reduction in left ventricular remodeling [98]. In addition to anakinra, there are two biologics that reduce IL-1α activity: bermekimab and rilonacept. Bermekimab acts as a monoclonal antibody and rilonacept is IL-1 soluble receptor. Anakinra and rilonacept block IL-1α and reduce IL-1β activity, while bermekimab is specific for IL-1α [99]. There remain plentiful drugs that inhibit the secretion of pro-inflammatory cytokines. Recent studies have shown that drugs that can reduce both IL-1β and TNF-α levels include metformin, L-carnitine, resveratrol (RSV), the Gal-3 inhibitor modified citrus pectin (MCP), and Biochanin A, among others [100,101,102,103,104].
Promotion of secretion of pro-angiogenic factors
As is well known, VEGF promotes angiogenesis. However, because of the short half-life and fast clearance rate of VEGF in vivo, it has been difficult to use it in sustained and effective treatments. Therefore, over the years, there have been investigations of various treatment options to increase VEGF concentration in the cardiovascular system. One of the more mature treatments is VEGF nanoparticle technology. At present, VEGF nanoparticles can release VEGF continuously for 31 days or more. When the density of blood vessels around the infarct area increases, the administration of VEGF nanoparticles increases accordingly, which can ultimately reduce the size of MI in mice and improve left ventricular systolic function [105, 106]. In addition, there have also been advances in gene therapy. Therapy with the Elabela gene activates the VEFG/VEGFR2 and Jagged1/Notch3 pathways through APJ, which promotes angiogenesis after MI [107]. Similarly, there are corresponding treatment regimens for VEGF-A and VEGF-B. Studies have found that Annexin A1 can directly promote cardiac macrophage polarization and stimulate release of large amounts of VEGF-A, which in turn induces neovascularization and repair of cardiomyocytes [108]. In addition, as a naturally polyphenolic phytoalexin, not only does RSV alleviate myocardial IRI by upregulating VEGF-B through the VEGF-B/AMPK/eNOS/NO signaling pathway, it can play a protective effect against isoproterenol-induced MI [109].
TGF-β is widely regarded as the "master switch" that mediates progression of the infarct from the inflammatory stage to scarring, playing a key role in remodeling myocardial tissue [110]. Therefore, in contrast to the goal of reducing TGF-β levels when treating tumors, we should increase TGF-β levels to promote development of collateral circulation. Although significant progress has been made in clinical trials targeting TGF-β, and many drugs have been developed to inhibit or block TGF-β synthesis, binding to receptors, and signaling pathways [111], there have been relatively few studies of treatments that increase TGF-β levels. Grundmann et al. [112] were the first to report the successful use of intravascular stents to release pro-arteriogenic compounds in a rabbit model. A bio-erodible polymer was coated on the endovascular stent, and TGF-β1 was then continuously released into the arterial lumen, which increased local plasma levels of TGF-β1 and stimulated collateral arteriogenesis [112]. However, because TGF-β1/Smads is a key signaling pathway in cardiac fibrosis, a novel therapeutic strategy has been to target inhibition of the AMPK-TGF-β1/Smads pathway to modulate remodeling after MI. The latest study found that Empagliflozin, which acts as a sodium-glucose cotransporter 2 inhibitor (SGLT2i), can inhibit the TGF-β1/Smad3 pathway and reduce collagen formation and myocardial fibrosis. In clinical practice, it can significantly reduce the number of cardiovascular deaths and the hospitalization rate for heart failure [113, 114]. Additionally, inhibition of tissue-nonspecific alkaline phosphatase (TNAP) also inhibits the TGF-β1/Smads pathway and may be a novel regulator of cardiac fibrosis [77].
Regulation of related signaling pathways
The JAK/STAT pathway is a post-stress inflammatory signaling pathway that mediates the growth, survival and apoptosis of cardiomyocytes and is also involved in regulation of angiogenesis. Hyaluronic acid oligosaccharide (o-HA) mainly stimulates expression of the JAK/STAT signaling pathway, which can reduce infarct size and promote angiogenesis of myocardium and reconstruction of myocardial function. Studies have shown that o-HA can stimulate expression of the chemokines Ccl2 and Cxcl5, promote polarization of macrophages, and enhance the MAPK and JAK/STAT signaling pathways to achieve a compensatory response to myocardial dysfunction. After treatment, the number of new blood vessels in damaged areas increases [115]. Losartan, tofacitinib, AG-490, and similar drugs are able to inhibit expression of the JAK/STAT signaling pathway. Among them, losartan can completely inhibit the increase in p-JAK2 and p-STAT3 after Ang II stimulation of cardiomyocytes, thereby repressing expression of the JAK/STAT pathway in the infarcted area [39]. Tofacitinib can inhibit angiogenesis by reducing the activity of JAK3 [116]. The tyrosine kinase inhibitor AG-490 has proven to be a selective inhibitor of JAK2 that reduces Ang II and platelet-derived growth factor (PDGF)-induced proliferation of arterial smooth muscle cells [40, 117]. Additionally, AG490 inhibits STAT3 activation and blocks NR4A3-mediated inhibition of NF-κB pathway activation [118].
NF-κB is a typical pro-inflammatory signaling pathway that promotes inflammatory responses by regulating gene transcription. Many drugs that play an anti-inflammatory role by inhibiting the NF-κB signaling pathway have been extensively studied. For example, latifolin and astragaloside IV can regulate expression of NF-κB. The former inhibits the inflammatory response of macrophages by regulating the HIF-1α/NF-κB/IL-6 signaling pathway, and the latter regulates TLR4/NF-κB/PPAR signaling-mediated energy biosynthesis to alleviate LPS-induced myocardial injury [119, 120]. In addition, morroniside, NR4A3 and metformin can suppress expression of NF-κB. Among them, morroniside can reduce expression of adhesion molecules, pro-inflammatory cytokines, chemokines, inflammatory receptors and other substances by reducing expression of NF-κB [121]. Similarly, NR4A3 inhibits NF-κB activation and inflammatory cell infiltration, thereby reducing acute ischemic injury of cardiomyocytes [118]. In addition, the AMPK agonist metformin reduces JNK and downstream NF-κB activation and reduces ROS production, thereby inhibiting the inflammatory response induced by JNK-NF-κB cascade signaling [122].
Following AMI, PI3K is an important protective pathway that can regulate cell proliferation, differentiation, migration and apoptosis. The lysyl oxidase-like protein 2 (LOXL2) triggers myo-fibroblast transformation and enhances collagen fiber production and mechanical strength by stimulating the PI3K-AKT-mTOR pathway [123]. By contrast, ivabradine suppresses PI3K/AKT/mTOR/p70S6K signaling to prevent fibrosis and cardiac hypertrophy [124, 125].
Conclusion
A growing number of studies have revealed that MI may induce a cytokine storm, for which we believe the key cytokines are IL-1, IL-6, IL-12, TNF-α, VEGF, MCP-1 and TGF-β. They can be roughly divided into two categories based on function: protective cytokines and damaging cytokines. They affect the prognosis of heart conditions by regulating regeneration and remodeling of CCC. Cytokines play a protective role in the compensatory phase of MI. Not only can they stimulate migration and proliferation of coronary vascular ECs and VSMCs but they can also promote activation of fibroblasts and differentiation and aggregation of immune cells. After the myocardial oxygen supply is decompensated, cytokine activation increases greatly and produces a cytokine storm. The overall damaging effects of cytokines is far greater than their protective effects, and they ultimately induce cardiomyocyte apoptosis, which significantly limits recovery of cardiac function. Due to the different types and levels of cytokines activated in a cytokine storm in different patients, regeneration of collateral circulation is heterogeneous. Therefore, cytokines or cytokine inhibitors may become an important weapon to improve the prognosis of patients with MI. Moreover, it has been shown that progression of a variety of acute and critical diseases is related to cytokine storms. Thus, we are confident that cytokine therapy will become an important tool for overcoming diseases in future.
References
World Health Organization. The top 10 causes of death. 2020. [accessed 2022 Feb 18]. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
Timmis A, Vardas P, Townsend N, Torbica A, Katus H, De Smedt D, Gale CP, Maggioni AP, Petersen SE, Huculeci R, Kazakiewicz D, de Benito Rubio V, Ignatiuk B, Raisi-Estabragh Z, Pawlak A, Karagiannidis E, Treskes R, Gaita D, Beltrame JF, McConnachie A, Bardinet I, Graham I, Flather M, Elliott P, Mossialos EA, Weidinger F, Achenbach S, Atlas Writing Group ESoC. European Society of Cardiology: cardiovascular disease statistics 2021. Eur Heart J 2022;43:716–799.
Zeymer U, Ludman P, Danchin N, Kala P, Laroche C, Sadeghi M, Caporale R, Shaheen SM, Legutko J, Iakobsishvili Z, Alhabib KF, Motovska Z, Studencan M, Mimoso J, Becker D, Alexopoulos D, Kereseselidze Z, Stojkovic S, Zelveian P, Goda A, Mirrakhimov E, Bajraktari G, Al-Farhan H, Šerpytis P, Raungaard B, Marandi T, Moore AM, Quinn M, Karjalainen PP, Tatu-Chitolu G, Gale CP, Maggioni AP, Weidinger F. Reperfusion therapies and in-hospital outcomes for ST-elevation myocardial infarction in Europe: the ACVC-EAPCI EORP STEMI Registry of the European Society of Cardiology. Eur Heart J. 2021;42:4536–49.
Shao C, Wang J, Tian J, Tang YD. Coronary artery disease: from mechanism to clinical practice. Adv Exp Med Biol. 2020;1177:1–36.
The World Bank. Toward a healthy and harmonious life in China: Stemming the rising of non-communicable diseases. 2011. [accessed 2022 Feb 27]. Available from: http://www.worldbank.org/content/dam/Worldbank/document/NCD_report_en.pdf.
Song J, Murugiah K, Hu S, Gao Y, Li X, Krumholz HM, Zheng X. Incidence, predictors, and prognostic impact of recurrent acute myocardial infarction in China. Heart. 2020;107:313–8.
Guan W, Venkatesh AK, Bai X, Xuan S, Li J, Li X, Zhang H, Zheng X, Masoudi FA, Spertus JA, Krumholz HM, Jiang L. Time to hospital arrival among patients with acute myocardial infarction in China: a report from China PEACE prospective study. Eur Heart J Qual Care Clin Outcomes. 2018;5:63–71.
Mahmud E, Dauerman HL, Welt FGP, Messenger JC, Rao SV, Grines C, Mattu A, Kirtane AJ, Jauhar R, Meraj P, Rokos IC, Rumsfeld JS, Henry TD. Management of acute myocardial infarction during the COVID-19 pandemic: A consensus statement from the society for cardiovascular angiography and interventions (SCAI), the American College of Cardiology (ACC), and the American College of Emergency Physicians (ACEP). Catheter Cardiovasc Interv. 2020;96:336–45.
Mizera L, Borst O. COVID-19 and the incidence of acute myocardial injury. Hamostaseologie. 2021;41:356–64.
Hausenloy DJ, Chilian W, Crea F, Davidson SM, Ferdinandy P, Garcia-Dorado D, van Royen N, Schulz R, Heusch G. The coronary circulation in acute myocardial ischaemia/reperfusion injury: a target for cardioprotection. Cardiovasc Res. 2019;115:1143–55.
Rakhit RD, Seiler C, Wustmann K, Zbinden S, Windecker S, Meier B, Eberli FR. Tumour necrosis factor-alpha and interleukin-6 release during primary percutaneous coronary intervention for acute myocardial infarction is related to coronary collateral flow. Coron Artery Dis. 2005;16:147–52.
Zimarino M, D’Andreamatteo M, Waksman R, Epstein SE, De Caterina R. The dynamics of the coronary collateral circulation. Nat Rev Cardiol. 2014;11:191–7.
Liu X, Liu Z, Chen J, Zhu L, Zhang H, Quan X, Yuan Y, Miao H, Huang B, Dong H, Zhang Z. Pigment epithelium-derived factor increases native collateral blood flow to improve cardiac function and induce ventricular remodeling after acute myocardial infarction. J Am Heart Assoc. 2019;8: e013323.
Werner GS, Ferrari M, Betge S, Gastmann O, Richartz BM, Figulla HR. Collateral function in chronic total coronary occlusions is related to regional myocardial function and duration of occlusion. Circulation. 2001;104:2784–90.
Seiler C, Stoller M, Pitt B, Meier P. The human coronary collateral circulation: development and clinical importance. Eur Heart J. 2013;34:2674–82.
Risau W. Mechanisms of angiogenesis. Nature. 1997;386:671–4.
van der Hoeven NW, Teunissen PF, Werner GS, Delewi R, Schirmer SH, Traupe T, van der Laan AM, Tijssen JG, Piek JJ, Seiler C, van Royen N. Clinical parameters associated with collateral development in patients with chronic total coronary occlusion. Heart. 2013;99:1100–5.
Steg PG, Kerner A, Mancini GB, Reynolds HR, Carvalho AC, Fridrich V, White HD, Forman SA, Lamas GA, Hochman JS, Buller CE. Impact of collateral flow to the occluded infarct-related artery on clinical outcomes in patients with recent myocardial infarction: a report from the randomized occluded artery trial. Circulation. 2010;121:2724–30.
Kim EK, Choi JH, Song YB, Hahn JY, Chang SA, Park SJ, Lee SC, Choi SH, Choe YH, Park SW, Gwon HC. A protective role of early collateral blood flow in patients with ST-segment elevation myocardial infarction. Am Heart J. 2016;171:56–63.
Das S, Goldstone AB, Wang H, Farry J, D’Amato G, Paulsen MJ, Eskandari A, Hironaka CE, Phansalkar R, Sharma B, Rhee S, Shamskhou EA, Agalliu D, de Jesus PV, Woo YJ, Red-Horse K. A unique collateral artery development program promotes neonatal heart regeneration. Cell. 2019;176:1128-1142.e1118.
Park HJ, Chang K, Park CS, Jang SW, Ihm SH, Kim PJ, Baek SH, Seung KB, Choi KB. Coronary collaterals: the role of MCP-1 during the early phase of acute myocardial infarction. Int J Cardiol. 2008;130:409–13.
Meier P, Gloekler S, de Marchi SF, Indermuehle A, Rutz T, Traupe T, Steck H, Vogel R, Seiler C. Myocardial salvage through coronary collateral growth by granulocyte colony-stimulating factor in chronic coronary artery disease: a controlled randomized trial. Circulation. 2009;120:1355–63.
Wang W, Yang ZJ, Ma DC, Wang LS, Xu SL, Zhang YR, Cao KJ, Zhang FM, Ma WZ. Induction of collateral artery growth and improvement of post-infarct heart function by hepatocyte growth factor gene transfer. Acta Pharmacol Sin. 2006;27:555–60.
Fajgenbaum DC, June CH. Cytokine storm. N Engl J Med. 2020;383:2255–73.
Wang X, Guo Z, Ding Z, Mehta JL. Inflammation, Autophagy, and Apoptosis After Myocardial Infarction. J Am Heart Assoc. 2018. https://doi.org/10.1161/JAHA.117.008024.
Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014;11:255–65.
Ma Y. Role of Neutrophils in Cardiac Injury and Repair Following Myocardial Infarction. Cells. 2021;10:1676.
Bradshaw PC, Seeds WA, Miller AC, Mahajan VR, Curtis WM. COVID-19: proposing a ketone-based metabolic therapy as a treatment to blunt the cytokine storm. Oxid Med Cell Longev. 2020;2020:6401341.
Hartman MHT, Groot HE, Leach IM, Karper JC, van der Harst P. Translational overview of cytokine inhibition in acute myocardial infarction and chronic heart failure. Trends Cardiovasc Med. 2018;28:369–79.
Shahrivari M, Wise E, Resende M, Shuster JJ, Zhang J, Bolli R, Cooke JP, Hare JM, Henry TD, Khan A, Taylor DA, Traverse JH, Yang PC, Pepine CJ, Cogle CR. Peripheral blood cytokine levels after acute myocardial infarction: IL-1β- and IL-6-related impairment of bone marrow function. Circ Res. 2017;120:1947–57.
Hwang MW, Matsumori A, Furukawa Y, Ono K, Okada M, Iwasaki A, Hara M, Miyamoto T, Touma M, Sasayama S. Neutralization of interleukin-1beta in the acute phase of myocardial infarction promotes the progression of left ventricular remodeling. J Am Coll Cardiol. 2001;38:1546–53.
Li Z, Hu S, Huang K, Su T, Cores J, Cheng K. Targeted anti-IL-1β platelet microparticles for cardiac detoxing and repair. Sci Adv 2020;6:eaay0589.
Guillén I, Blanes M, Gómez-Lechón MJ, Castell JV. Cytokine signaling during myocardial infarction: sequential appearance of IL-1 beta and IL-6. Am J Physiol. 1995;269:R229-235.
Abbate A, Salloum FN, Van Tassell BW, Vecile E, Toldo S, Seropian I, Mezzaroma E, Dobrina A. Alterations in the interleukin-1/interleukin-1 receptor antagonist balance modulate cardiac remodeling following myocardial infarction in the mouse. PLoS ONE. 2011;6: e27923.
Garbers C, Aparicio-Siegmund S, Rose-John S. The IL-6/gp130/STAT3 signaling axis: recent advances towards specific inhibition. Curr Opin Immunol. 2015;34:75–82.
Kang S, Narazaki M, Metwally H, Kishimoto T. Historical overview of the interleukin-6 family cytokine. J Exp Med. 2020. https://doi.org/10.1084/jem.20190347.
Scheller J, Chalaris A, Schmidt-Arras D, Rose-John S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim Biophys Acta. 2011;1813:878–88.
Xu H, Yang YJ, Qian HY, Tang YD, Wang H, Zhang Q. Rosuvastatin treatment activates JAK-STAT pathway and increases efficacy of allogeneic mesenchymal stem cell transplantation in infarcted hearts. Circ J. 2011;75:1476–85.
Xin LH, Liu R, Yang XW. Losartan promotes myocardial apoptosis after acute myocardial infarction in rats through inhibiting Ang II-induced JAK/STAT pathway. Eur Rev Med Pharmacol Sci. 2020;24:409–17.
Zhang S, Liu X, Goldstein S, Li Y, Ge J, He B, Fei X, Wang Z, Ruiz G. Role of the JAK/STAT signaling pathway in the pathogenesis of acute myocardial infarction in rats and its effect on NF-κB expression. Mol Med Rep. 2013;7:93–8.
Krylatov AV, Maslov LN, Voronkov NS, Boshchenko AA, Popov SV, Gomez L, Wang H, Jaggi AS, Downey JM. Reactive oxygen species as intracellular signaling molecules in the cardiovascular system. Curr Cardiol Rev. 2018;14:290–300.
Kan X, Wu Y, Ma Y, Zhang C, Li P, Wu L, Zhang S, Li Y, Du J. Deficiency of IL-12p35 improves cardiac repair after myocardial infarction by promoting angiogenesis. Cardiovasc Res. 2016;109:249–59.
Thierfelder WE, van Deursen JM, Yamamoto K, Tripp RA, Sarawar SR, Carson RT, Sangster MY, Vignali DA, Doherty PC, Grosveld GC, Ihle JN. Requirement for Stat4 in interleukin-12-mediated responses of natural killer and T cells. Nature. 1996;382:171–4.
Correia LC, Andrade BB, Borges VM, Clarêncio J, Bittencourt AP, Freitas R, Souza AC, Almeida MC, Leal J, Esteves JP, Barral-Netto M. Prognostic value of cytokines and chemokines in addition to the GRACE Score in non-ST-elevation acute coronary syndromes. Clin Chim Acta. 2010;411:540–5.
Selzman CH, Shames BD, Reznikov LL, Miller SA, Meng X, Barton HA, Werman A, Harken AH, Dinarello CA, Banerjee A. Liposomal delivery of purified inhibitory-kappaBalpha inhibits tumor necrosis factor-alpha-induced human vascular smooth muscle proliferation. Circ Res. 1999;84:867–75.
Irwin MW, Mak S, Mann DL, Qu R, Penninger JM, Yan A, Dawood F, Wen WH, Shou Z, Liu P. Tissue expression and immunolocalization of tumor necrosis factor-alpha in postinfarction dysfunctional myocardium. Circulation. 1999;99:1492–8.
Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E. Elevation of tumor necrosis factor-alpha and increased risk of recurrent coronary events after myocardial infarction. Circulation. 2000;101:2149–53.
Neri M, Fineschi V, Di Paolo M, Pomara C, Riezzo I, Turillazzi E, Cerretani D. Cardiac oxidative stress and inflammatory cytokines response after myocardial infarction. Curr Vasc Pharmacol. 2015;13:26–36.
Ho FM, Lin WW, Chen BC, Chao CM, Yang CR, Lin LY, Lai CC, Liu SH, Liau CS. High glucose-induced apoptosis in human vascular endothelial cells is mediated through NF-kappaB and c-Jun NH2-terminal kinase pathway and prevented by PI3K/Akt/eNOS pathway. Cell Signal. 2006;18:391–9.
Lawrence T. The nuclear factor NF-kappaB pathway in inflammation. Cold Spring Harb Perspect Biol. 2009;1: a001651.
Onai Y, Suzuki J, Maejima Y, Haraguchi G, Muto S, Itai A, Isobe M. Inhibition of NF-{kappa}B improves left ventricular remodeling and cardiac dysfunction after myocardial infarction. Am J Physiol Heart Circ Physiol. 2007;292:H530-538.
Natoli G, Costanzo A, Moretti F, Fulco M, Balsano C, Levrero M. J Biol Chem. 1997;272:26079–82.
Morgan MJ, Liu ZG. Reactive oxygen species in TNFalpha-induced signaling and cell death. Mol Cells. 2010;30:1–12.
Hori M, Nishida K. Oxidative stress and left ventricular remodelling after myocardial infarction. Cardiovasc Res. 2009;81:457–64.
Sun Y, Wang S, Zhao L, Zhang B, Chen H. IFN-γ and TNF-α aggravate endothelial damage caused by CD123-targeted CAR T cell. Onco Targets Ther. 2019;12:4907–25.
Aggarwal BB, Gupta SC, Kim JH. Historical perspectives on tumor necrosis factor and its superfamily: 25 years later, a golden journey. Blood. 2012;119:651–65.
Song X, Qian Y. The activation and regulation of IL-17 receptor mediated signaling. Cytokine. 2013;62:175–82.
Peach CJ, Mignone VW, Arruda MA, Alcobia DC, Hill SJ, Kilpatrick LE, Woolard J. Molecular Pharmacology of VEGF-A Isoforms: Binding and Signalling at VEGFR2. Int J Mol Sci. 2018;19:1264.
Liu D, Song J, Ji X, Liu Z, Cong M, Hu B. Association of genetic Polymorphisms on VEGFA and VEGFR2 with risk of coronary heart disease. Medicine (Baltimore). 2016;95: e3413.
Gerber HP, McMurtrey A, Kowalski J, Yan M, Keyt BA, Dixit V, Ferrara N. Vascular endothelial growth factor regulates endothelial cell survival through the phosphatidylinositol 3’-kinase/Akt signal transduction pathway. Requirement for Flk-1/KDR activation. J Biol Chem. 1998;273:30336–43.
McMullen ME, Bryant PW, Glembotski CC, Vincent PA, Pumiglia KM. Activation of p38 has opposing effects on the proliferation and migration of endothelial cells. J Biol Chem. 2005;280:20995–1003.
Chen XL, Nam JO, Jean C, Lawson C, Walsh CT, Goka E, Lim ST, Tomar A, Tancioni I, Uryu S, Guan JL, Acevedo LM, Weis SM, Cheresh DA, Schlaepfer DD. VEGF-induced vascular permeability is mediated by FAK. Dev Cell. 2012;22:146–57.
Takahashi T, Yamaguchi S, Chida K, Shibuya M. A single autophosphorylation site on KDR/Flk-1 is essential for VEGF-A-dependent activation of PLC-gamma and DNA synthesis in vascular endothelial cells. Embo j. 2001;20:2768–78.
Takahashi T, Ueno H, Shibuya M. VEGF activates protein kinase C-dependent, but Ras-independent Raf-MEK-MAP kinase pathway for DNA synthesis in primary endothelial cells. Oncogene. 1999;18:2221–30.
Yang B, Yan P, Gong H, Zuo L, Shi Y, Guo J, Guo R, Xie J, Li B. TWEAK protects cardiomyocyte against apoptosis in a PI3K/AKT pathway dependent manner. Am J Transl Res. 2016;8:3848–60.
Zou J, Fei Q, Xiao H, Wang H, Liu K, Liu M, Zhang H, Xiao X, Wang K, Wang N. VEGF-A promotes angiogenesis after acute myocardial infarction through increasing ROS production and enhancing ER stress-mediated autophagy. J Cell Physiol. 2019;234:17690–703.
Kobusiak-Prokopowicz M, Orzeszko J, Mazur G, Mysiak A, Orda A, Poreba R, Mazurek W. Chemokines and left ventricular function in patients with acute myocardial infarction. Eur J Intern Med. 2007;18:288–94.
Sahinarslan A, Kocaman SA, Topal S, Ercin U, Bukan N, Yalcin R, Timurkaynak T. Relation between serum monocyte chemoattractant protein-1 and coronary collateral development. Coron Artery Dis. 2010;21:455–9.
Morimoto H, Takahashi M, Izawa A, Ise H, Hongo M, Kolattukudy PE, Ikeda U. Cardiac overexpression of monocyte chemoattractant protein-1 in transgenic mice prevents cardiac dysfunction and remodeling after myocardial infarction. Circ Res. 2006;99:891–9.
Frangogiannis NG, Dewald O, Xia Y, Ren G, Haudek S, Leucker T, Kraemer D, Taffet G, Rollins BJ, Entman ML. Critical role of monocyte chemoattractant protein-1/CC chemokine ligand 2 in the pathogenesis of ischemic cardiomyopathy. Circulation. 2007;115:584–92.
Dewald O, Zymek P, Winkelmann K, Koerting A, Ren G, Abou-Khamis T, Michael LH, Rollins BJ, Entman ML, Frangogiannis NG. CCL2/Monocyte Chemoattractant protein-1 regulates inflammatory responses critical to healing myocardial infarcts. Circ Res. 2005;96:881–9.
Weir RA, Murphy CA, Petrie CJ, Martin TN, Clements S, Steedman T, Wagner GS, McMurray JJ, Dargie HJ. Monocyte chemoattractant protein-1: a dichotomous role in cardiac remodeling following acute myocardial infarction in man? Cytokine. 2010;50:158–62.
França CN, Izar MCO, Hortêncio MNS, do Amaral JB, Ferreira CES, Tuleta ID, Fonseca FAH. Monocyte subtypes and the CCR2 chemokine receptor in cardiovascular disease. Clin Sci (Lond) 2017;131:1215–1224.
Khalil H, Kanisicak O, Prasad V, Correll RN, Fu X, Schips T, Vagnozzi RJ, Liu R, Huynh T, Lee SJ, Karch J, Molkentin JD. Fibroblast-specific TGF-β-Smad2/3 signaling underlies cardiac fibrosis. J Clin Invest. 2017;127:3770–83.
Meng XM, Nikolic-Paterson DJ, Lan HY. TGF-β: the master regulator of fibrosis. Nat Rev Nephrol. 2016;12:325–38.
Ma J, Li ZY, Liang XP, Guo CX, Lu PP, Ma LH. Xinfuli Granule improves post-myocardial infarction ventricular remodeling and myocardial fibrosis in rats by regulating TGF-β/Smads signaling pathway. J Geriatr Cardiol. 2017;14:301–7.
Gao L, Wang LY, Liu ZQ, Jiang D, Wu SY, Guo YQ, Tao HM, Sun M, You LN, Qin S, Cheng XC, Xie JS, Chang GL, Zhang DY. TNAP inhibition attenuates cardiac fibrosis induced by myocardial infarction through deactivating TGF-β1/Smads and activating P53 signaling pathways. Cell Death Dis. 2020;11:44.
Bujak M, Frangogiannis NG. The role of TGF-beta signaling in myocardial infarction and cardiac remodeling. Cardiovasc Res. 2007;74:184–95.
Chillo O, Kleinert EC, Lautz T, Lasch M, Pagel JI, Heun Y, Troidl K, Fischer S, Caballero-Martinez A, Mauer A, Kurz ARM, Assmann G, Rehberg M, Kanse SM, Nieswandt B, Walzog B, Reichel CA, Mannell H, Preissner KT, Deindl E. Perivascular mast cells govern shear stress-induced arteriogenesis by orchestrating leukocyte function. Cell Rep. 2016;16:2197–207.
Lasch M, Kleinert EC, Meister S, Kumaraswami K, Buchheim JI, Grantzow T, Lautz T, Salpisti S, Fischer S, Troidl K, Fleming I, Randi AM, Sperandio M, Preissner KT, Deindl E. Extracellular RNA released due to shear stress controls natural bypass growth by mediating mechanotransduction in mice. Blood. 2019;134:1469–79.
Kluever AK, Braumandl A, Fischer S, Preissner KT, Deindl E. The extraordinary role of extracellular rna in arteriogenesis, the growth of collateral arteries. Int J Mol Sci. 2019;20:6177.
Cook-Mills JM. VCAM-1 signals during lymphocyte migration: role of reactive oxygen species. Mol Immunol. 2002;39:499–508.
Deem TL, Abdala-Valencia H, Cook-Mills JM. VCAM-1 activation of endothelial cell protein tyrosine phosphatase 1B. J Immunol. 2007;178:3865–73.
Kang S, Kishimoto T. Interplay between interleukin-6 signaling and the vascular endothelium in cytokine storms. Exp Mol Med. 2021;53:1116–23.
Li W, Liu C, Burns N, Hayashi J, Yoshida A, Sajja A, González-Hernández S, Gao JL, Murphy PM, Kubota Y, Zou YR, Nagasawa T, Mukouyama YS. Alterations in the spatiotemporal expression of the chemokine receptor CXCR4 in endothelial cells cause failure of hierarchical vascular branching. Dev Biol. 2021;477:70–84.
Gu Q, Yang XP, Bonde P, DiPaula A, Fox-Talbot K, Becker LC. Inhibition of TNF-alpha reduces myocardial injury and proinflammatory pathways following ischemia-reperfusion in the dog. J Cardiovasc Pharmacol. 2006;48:320–8.
de Rivero Vaccari JC, Dietrich WD, Keane RW, de Rivero Vaccari JP. The inflammasome in times of COVID-19. Front Immunol. 2020;11: 583373.
Chu H, Wang Y. Therapeutic angiogenesis: controlled delivery of angiogenic factors. Ther Deliv. 2012;3:693–714.
Xu Y, Tang T, Ding Y, Yao R, Xie J, Liao M, Xiao H, Chen Y, Yu X, Fu M, Liao Y, Zhao G, Cheng X. Improved cardiac performance by rosuvastatin is associated with attenuations in both myocardial tumor necrosis factor-alpha and p38 MAP kinase activity in rats after myocardial infarction. Am J Med Sci. 2010;340:121–7.
Bao JW, Sun B, Ma PP, Gai YS, Sun WZ, Yu HQ, Li J. Rosuvastatin inhibits inflammatory response and resists fibrosis after myocardial infarction. Eur Rev Med Pharmacol Sci. 2018;22:238–45.
Zaitone SA, Abo-Gresha NM. Rosuvastatin promotes angiogenesis and reverses isoproterenol-induced acute myocardial infarction in rats: role of iNOS and VEGF. Eur J Pharmacol. 2012;691:134–42.
Rezaie-Majd A, Maca T, Bucek RA, Valent P, Müller MR, Husslein P, Kashanipour A, Minar E, Baghestanian M. Simvastatin reduces expression of cytokines interleukin-6, interleukin-8, and monocyte chemoattractant protein-1 in circulating monocytes from hypercholesterolemic patients. Arterioscler Thromb Vasc Biol. 2002;22:1194–9.
Li TS, Takahashi M, Suzuki R, Kobayashi T, Ito H, Mikamo A, Hamano K. Pravastatin improves remodeling and cardiac function after myocardial infarction by an antiinflammatory mechanism rather than by the induction of angiogenesis. Ann Thorac Surg. 2006;81:2217–25.
Lu W, Xie Z, Tang Y, Bai L, Yao Y, Fu C, Ma G. Photoluminescent Mesoporous silicon nanoparticles with siCCR2 improve the effects of mesenchymal stromal cell transplantation after acute myocardial infarction. Theranostics. 2015;5:1068–82.
Wang J, Seo MJ, Deci MB, Weil BR, Canty JM, Nguyen J. Effect of CCR2 inhibitor-loaded lipid micelles on inflammatory cell migration and cardiac function after myocardial infarction. Int J Nanomedicine. 2018;13:6441–51.
Liehn EA, Piccinini AM, Koenen RR, Soehnlein O, Adage T, Fatu R, Curaj A, Popescu A, Zernecke A, Kungl AJ, Weber C. A new monocyte chemotactic protein-1/chemokine CC motif ligand-2 competitor limiting neointima formation and myocardial ischemia/reperfusion injury in mice. J Am Coll Cardiol. 2010;56:1847–57.
Abbate A, Van Tassell BW, Biondi-Zoccai G, Kontos MC, Grizzard JD, Spillman DW, Oddi C, Roberts CS, Melchior RD, Mueller GH, Abouzaki NA, Rengel LR, Varma A, Gambill ML, Falcao RA, Voelkel NF, Dinarello CA, Vetrovec GW. Effects of interleukin-1 blockade with anakinra on adverse cardiac remodeling and heart failure after acute myocardial infarction [from the Virginia Commonwealth University-Anakinra Remodeling Trial (2) (VCU-ART2) pilot study]. Am J Cardiol. 2013;111:1394–400.
Dinarello CA, van der Meer JW. Treating inflammation by blocking interleukin-1 in humans. Semin Immunol. 2013;25:469–84.
Cavalli G, Colafrancesco S, Emmi G, Imazio M, Lopalco G, Maggio MC, Sota J, Dinarello CA. Interleukin 1α: a comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun Rev. 2021;20: 102763.
Zhang J, Huang L, Shi X, Yang L, Hua F, Ma J, Zhu W, Liu X, Xuan R, Shen Y, Liu J, Lai X, Yu P. Metformin protects against myocardial ischemia-reperfusion injury and cell pyroptosis via AMPK/NLRP3 inflammasome pathway. Aging (Albany NY). 2020;12:24270–87.
Emran T, Chowdhury NI, Sarker M, Bepari AK, Hossain M, Rahman GMS, Reza HM. L-carnitine protects cardiac damage by reducing oxidative stress and inflammatory response via inhibition of tumor necrosis factor-alpha and interleukin-1beta against isoproterenol-induced myocardial infarction. Biomed Pharmacother. 2021;143: 112139.
Feng H, Mou SQ, Li WJ, Zhang N, Zhou ZY, Ding W, Bian ZY, Liao HH. Resveratrol inhibits ischemia-induced myocardial senescence signals and NLRP3 inflammasome activation. Oxid Med Cell Longev. 2020;2020:2647807.
Xu GR, Zhang C, Yang HX, Sun JH, Zhang Y, Yao TT, Li Y, Ruan L, An R, Li AY. Modified citrus pectin ameliorates myocardial fibrosis and inflammation via suppressing galectin-3 and TLR4/MyD88/NF-κB signaling pathway. Biomed Pharmacother. 2020;126: 110071.
Bai Y, Li Z, Liu W, Gao D, Liu M, Zhang P. Biochanin A attenuates myocardial ischemia/reperfusion injury through the TLR4/NF-κB/NLRP3 signaling pathway. Acta Cir Bras. 2019;34: e201901104.
Oduk Y, Zhu W, Kannappan R, Zhao M, Borovjagin AV, Oparil S, Zhang JJ. VEGF nanoparticles repair the heart after myocardial infarction. Am J Physiol Heart Circ Physiol. 2018;314:H278-h284.
Awada HK, Johnson NR, Wang Y. Sequential delivery of angiogenic growth factors improves revascularization and heart function after myocardial infarction. J Control Release. 2015;207:7–17.
Jin L, Pan Y, Li Q, Li J, Wang Z. Elabela gene therapy promotes angiogenesis after myocardial infarction. J Cell Mol Med. 2021;25:8537–45.
Ferraro B, Leoni G, Hinkel R, Ormanns S, Paulin N, Ortega-Gomez A, Viola JR, de Jong R, Bongiovanni D, Bozoglu T, Maas SL, D’Amico M, Kessler T, Zeller T, Hristov M, Reutelingsperger C, Sager HB, Döring Y, Nahrendorf M, Kupatt C, Soehnlein O. Pro-angiogenic macrophage phenotype to promote myocardial repair. J Am Coll Cardiol. 2019;73:2990–3002.
Feng L, Ren J, Li Y, Yang G, Kang L, Zhang S, Ma C, Li J, Liu J, Yang L, Qi Z. Resveratrol protects against isoproterenol induced myocardial infarction in rats through VEGF-B/AMPK/eNOS/NO signalling pathway. Free Radic Res. 2019;53:82–93.
Dobaczewski M, Chen W, Frangogiannis NG. Transforming growth factor (TGF)-β signaling in cardiac remodeling. J Mol Cell Cardiol. 2011;51:600–6.
Haque S, Morris JC. Transforming growth factor-β: A therapeutic target for cancer. Hum Vaccin Immunother. 2017;13:1741–50.
Grundmann S, van Royen N, Pasterkamp G, Gonzalez N, Tijsma EJ, Piek JJ, Hoefer IE. A new intra-arterial delivery platform for pro-arteriogenic compounds to stimulate collateral artery growth via transforming growth factor-beta1 release. J Am Coll Cardiol. 2007;50:351–8.
Daud E, Ertracht O, Bandel N, Moady G, Shehadeh M, Reuveni T, Atar S. The impact of empagliflozin on cardiac physiology and fibrosis early after myocardial infarction in non-diabetic rats. Cardiovasc Diabetol. 2021;20:132.
Kang S, Verma S, Hassanabad AF, Teng G, Belke DD, Dundas JA, Guzzardi DG, Svystonyuk DA, Pattar SS, Park DSJ, Turnbull JD, Duff HJ, Tibbles LA, Cunnington RH, Dyck JRB, Fedak PWM. Direct effects of empagliflozin on extracellular matrix remodelling in human cardiac myofibroblasts: novel translational clues to explain EMPA-REG outcome results. Can J Cardiol. 2020;36:543–53.
Wang N, Liu C, Wang X, He T, Li L, Liang X, Wang L, Song L, Wei Y, Wu Q, Gong C. Hyaluronic acid oligosaccharides improve myocardial function reconstruction and angiogenesis against myocardial infarction by regulation of macrophages. Theranostics. 2019;9:1980–92.
López-Sanromán A, Esplugues JV, Domènech E. Pharmacology and safety of tofacitinib in ulcerative colitis. Gastroenterol Hepatol. 2021;44:39–48.
Meydan N, Grunberger T, Dadi H, Shahar M, Arpaia E, Lapidot Z, Leeder JS, Freedman M, Cohen A, Gazit A, Levitzki A, Roifman CM. Inhibition of acute lymphoblastic leukaemia by a Jak-2 inhibitor. Nature. 1996;379:645–8.
Jiang Y, Feng YP, Tang LX, Yan YL, Bai JW. The protective role of NR4A3 in acute myocardial infarction by suppressing inflammatory responses via JAK2-STAT3/NF-κB pathway. Biochem Biophys Res Commun. 2019;517:697–702.
Lai XX, Zhang N, Chen LY, Luo YY, Shou BY, Xie XX, Liu RH. Latifolin protects against myocardial infarction by alleviating myocardial inflammatory via the HIF-1α/NF-κB/IL-6 pathway. Pharm Biol. 2020;58:1156–66.
Zhang X, Li M, Wang H. Astragaloside IV alleviates the myocardial damage induced by lipopolysaccharide via the toll-like receptor 4 (TLR4)/nuclear factor kappa B (NF-κB)/proliferator-activated receptor α (PPARα) Signaling Pathway. Med Sci Monit. 2019;25:7158–68.
Yu B, Wang W. Cardioprotective effects of morroniside in rats following acute myocardial infarction. Inflammation. 2018;41:432–6.
Chen X, Li X, Zhang W, He J, Xu B, Lei B, Wang Z, Cates C, Rousselle T, Li J. Activation of AMPK inhibits inflammatory response during hypoxia and reoxygenation through modulating JNK-mediated NF-κB pathway. Metabolism. 2018;83:256–70.
Yang J, Savvatis K, Kang JS, Fan P, Zhong H, Schwartz K, Barry V, Mikels-Vigdal A, Karpinski S, Kornyeyev D, Adamkewicz J, Feng X, Zhou Q, Shang C, Kumar P, Phan D, Kasner M, López B, Diez J, Wright KC, Kovacs RL, Chen PS, Quertermous T, Smith V, Yao L, Tschöpe C, Chang CP. Targeting LOXL2 for cardiac interstitial fibrosis and heart failure treatment. Nat Commun. 2016;7:13710.
Dai Y, Chen Y, Wei G, Zha L, Li X. Ivabradine protects rats against myocardial infarction through reinforcing autophagy via inhibiting PI3K/AKT/mTOR/p70S6K pathway. Bioengineered. 2021;12:1826–37.
Yu Y, Hu Z, Li B, Wang Z, Chen S. Ivabradine improved left ventricular function and pressure overload-induced cardiomyocyte apoptosis in a transverse aortic constriction mouse model. Mol Cell Biochem. 2019;450:25–34.
Funding
This work was supported by Guangdong Medical Science and Technology Research Foundation (A2020162, B2021182); Guangdong Basic and Applied Basic Research Foundation (2020A1515010288); Higher Education Teaching Reform Project of Southern Medical University (JG2019126, 2018JG43, JG2019130, JG201984); Social welfare and basic research project of Zhongshan City, Guangdong Province (2021B1090); Science and technology project of Zhaoqing City, Guangdong Province.
Author information
Authors and Affiliations
Contributions
PDZ conceptualized and designed the study. WH, PC and QC conducted the literature search and analysis, drafted the manuscript and contributed equally to this manuscript. All authors critically revised the manuscript and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflicts of interest
The authors have declared that no competing interest exists.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
He, W., Chen, P., Chen, Q. et al. Cytokine storm: behind the scenes of the collateral circulation after acute myocardial infarction. Inflamm. Res. 71, 1143–1158 (2022). https://doi.org/10.1007/s00011-022-01611-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-022-01611-0