Associations among Physician–Patient Communication, Patient Satisfaction, and Clinical Effectiveness of Overactive Bladder Medication: A Survey of Patients with Overactive Bladder


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Design
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patients
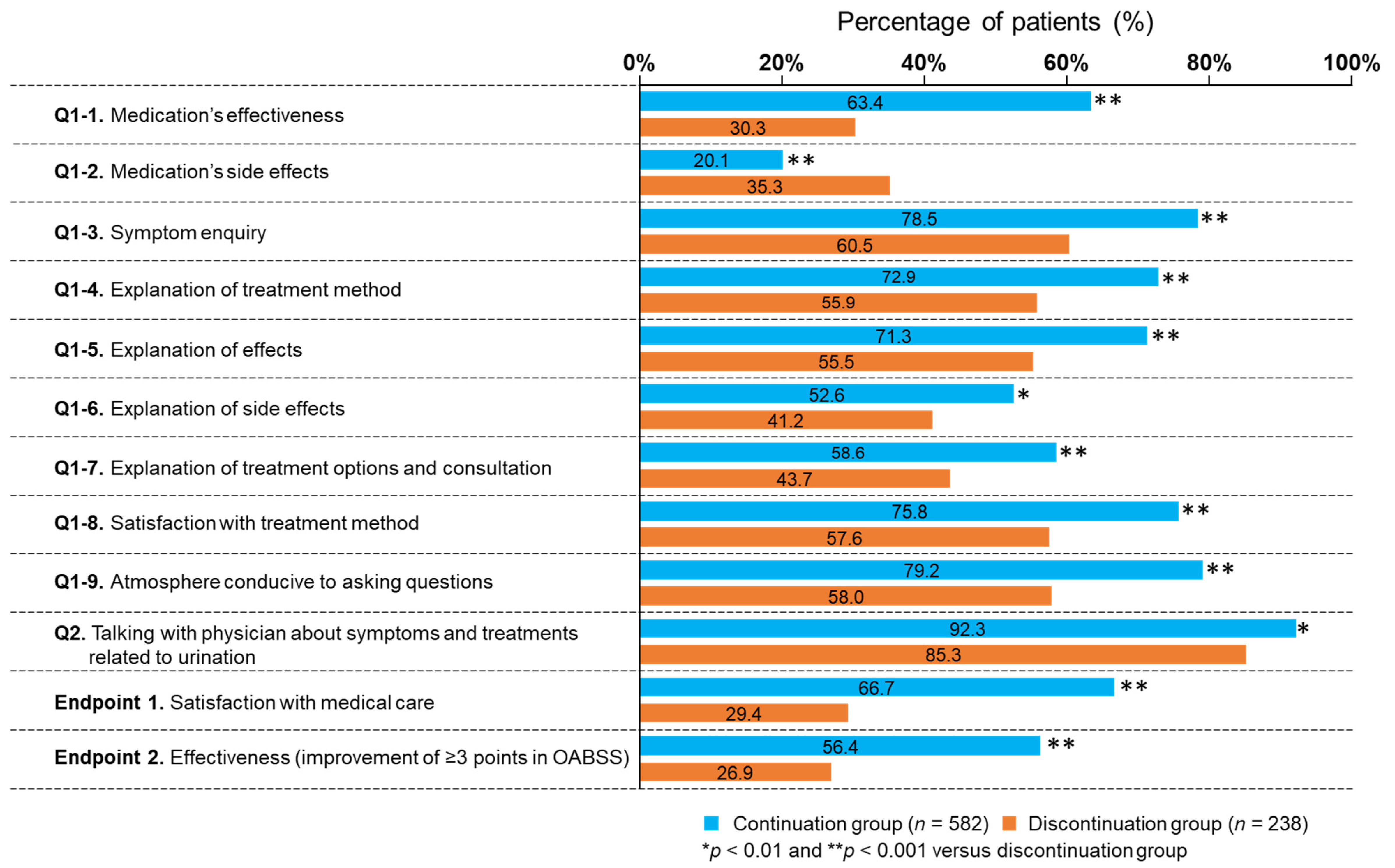
3.2. Survey Responses
3.3. Endpoints
3.4. Stratified Analyses in the Medication Discontinuation Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- American Urological Association. Diagnosis and Treatment of Non-Neurogenic Overactive Bladder (OAB) in Adults: An AUA/SUFU Guideline. 2019. Available online: https://www.auanet.org/guidelines/guidelines/overactive-bladder-(oab)-guideline (accessed on 22 April 2022).
- Homma, Y.; Yamaguchi, O.; Hayashi, K.; Neurogenic Bladder Society Committee. An epidemiological survey of overactive bladder symptoms in Japan. BJI Int. 2005, 96, 1314–1318. [Google Scholar] [CrossRef] [PubMed]
- Filipetto, F.; Fulda, K.; Holthusen, A.; McKeithen, T.M.; McFadden, P. The patient perspective on overactive bladder: A mixed-methods needs assessment. BMC Fam. Pract. 2014, 15, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dmochowski, R.; Newman, D. Impact of overactive bladder on women in the United States: Results of a national survey. Curr. Med. Res. Opin. 2007, 23, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Yeaw, J.; Benner, J.S.; Walt, J.G.; Sian, S.; Smith, D.B. Comparing adherence and persistence across 6 chronic medication classes. J. Manag. Care Pharm. 2009, 15, 728–740. [Google Scholar] [CrossRef] [PubMed]
- Yeowell, G.; Smith, P.; Nazir, J.; Hakimi, Z.; Siddiqui, E.; Fatoye, F. Real-world persistence and adherence to oral antimuscarinics and mirabegron in patients with overactive bladder (OAB): A systematic literature review. BMJ Open 2018, 8, e021889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haskard Zolnierek, K.B.; Dimatteo, M.R. Physician communication and patient adherence to treatment: A meta-analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homma, Y.; Yoshida, M.; Seki, N.; Yokoyama, O.; Kakizaki, H.; Gotoh, M.; Yamanishi, T.; Yamaguchi, O.; Takeda, M.; Nishizawa, O. Symptom assessment tool for overactive bladder syndrome—overactive bladder symptom score. Urology 2006, 68, 318. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Ethical Guidelines for Medical and Health Research Involving Human Subjects (English Translation, March 2015). Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf (accessed on 22 April 2022).
- Gotoh, M.; Homma, Y.; Yokoyama, O.; Nishizawa, O. Responsiveness and minimal clinically important change in overactive bladder symptom score. Urology 2011, 78, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.R.; Bradt, P.; Hewett, K.A.; Ng, D.B. Physician-patient communication about overactive bladder: Results of an observational sociolinguistic study. PLoS ONE 2017, 12, e0186122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, S.; Ito, Y.; Nishijima, S.; Kadekawa, K.; Sugaya, K. Basic and clinical aspects of antimuscarinic agents used to treat overactive bladder. Pharmacol. Ther. 2018, 189, 130–148. [Google Scholar] [CrossRef] [PubMed]
- Sussman, D.O.; Kraus, S.R.; Carlsson, M.; Guan, Z. Onset of efficacy of tolterodine extended release in patients with overactive bladder. Curr. Med. Res. Open 2007, 23, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.R.; Nitti, V.W.; Khullar, V.; Wyndaele, J.J.; Herschorn, S.; van Kerrebroeck, P.; Blauwet, M.B.; Siddiqui, E. Onset of action of the β3-adrenoceptor agonist, mirabegron, in Phase II and III clinical trials in patients with overactive bladder. World J. Urol. 2014, 32, 1565–1572. [Google Scholar] [CrossRef] [Green Version]
- Wagg, A.S.; Herschorn, S.; Carlsson, M.; Fernet, M.; Oelke, M. What are the chances of improvement or cure from overactive bladder? A pooled responder analysis of efficacy and treatment emergent adverse events following treatment with fesoterodine. Neurourol. Urodyn. 2021, 40, 1559–1568. [Google Scholar] [CrossRef] [PubMed]
- Marcelissen, T.; Rashid, T.; Lopes, T.A.; Delongchamps, N.B.; Geavlete, B.; Rieken, M.; Cornu, J.N.; Rahnama’i, M.S.; EAU Young Academic Urologists (YAU) functional urology working group. Oral pharmacologic management of overactive bladder syndrome: Where do we stand? Eur. Urol. Focus 2019, 5, 1112–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohloff, M.; Peifer, G.; Thompson, J.H. Patient navigation for overactive bladder improves access to care. Int. Urogynecol. J. 2020, 31, 1007–1012. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Population N = 1004 | ||
|---|---|---|
| Sex | ||
| Male | 591 | (58.9) |
| Female | 413 | (41.1) |
| Age, years | ||
| Mean (SD) | 70.3 | (7.1) |
| Median (IQR) | 71.0 | (10.0) |
| <70 years | 385 | (38.3) |
| ≥70 years | 619 | (61.7) |
| OABSS prior to medication | ||
| Mean (SD) | 9.0 | (2.6) |
| Median (IQR) | 9.0 | (4.0) |
| Change in OABSS | ||
| Mean (SD) | 3.1 | (2.9) |
| Median (IQR) | 3.0 | (4.0) |
| Clinically significant improvement in OABSS | ||
| Unimproved (<3 points) | 471 | (46.9) |
| Improved (≥3 points) | 533 | (53.1) |
| Medication adherence | ||
| Continued | 582 | (58.0) |
| Discontinued | 422 | (42.0) |
| Patient-reported reason for discontinuation | ||
| Symptom improvement | 184 | (43.6) |
| No symptom improvement | 116 | (27.5) |
| Worsening symptoms | 2 | (0.5) |
| Side effects | 46 | (10.9) |
| Used on an as needed basis | 63 | (14.9) |
| Other | 42 | (10.0) |
| Discontinued for any reason other than symptom improvement | 238 | (23.7) |
| Discontinued due to symptom improvement | 184 | (18.3) |
| Duration of medication exposure | ||
| <1 month | 70 | (7.0) |
| 1 to <3 months | 141 | (14.0) |
| 3 to <6 months | 141 | (14.0) |
| 6 to <12 months | 169 | (16.8) |
| ≥12 months | 483 | (48.1) |
| Switched medication | ||
| Yes | 387 | (38.5) |
| No | 617 | (61.5) |
| Department consulted | ||
| Urology | 733 | (73.0) |
| Internal medicine | 240 | (23.9) |
| Other | 26 | (2.6) |
| Unknown | 5 | (0.5) |
| Type of medical facility visited | ||
| Hospital | 391 | (38.9) |
| Clinic | 608 | (60.6) |
| Other | 5 | (0.5) |
| Comorbidities | ||
| Any | 730 | (72.7) |
| Hypertension | 413 | (41.1) |
| Dyslipidemia (hyperlipidemia) | 193 | (19.2) |
| Diabetes mellitus | 141 | (14.0) |
| Benign prostatic hyperplasia (male patients) | 277 | (46.9) |
| Other | 114 | (11.4) |
| None of the above | 274 | (27.3) |
| Explanatory Variables | p-Value | OR | 95% CI |
|---|---|---|---|
| Q1-1. Medication’s effectiveness | <0.001 | 7.99 | (5.59–11.43) |
| Q1-2. Medication’s side effects | <0.001 | 0.36 | (0.24–0.53) |
| Q1-3. Symptom enquiry | 0.56 | 1.16 | (0.70–1.92) |
| Q1-4. Explanation of treatment method | 0.26 | 1.34 | (0.81–2.24) |
| Q1-5. Explanation of effects | 0.37 | 1.25 | (0.76–2.07) |
| Q1-6. Explanation of side effects | 0.02 | 1.61 | (1.07–2.44) |
| Q1-7. Explanation of treatment options and consultation | 0.06 | 1.47 | (0.98–2.19) |
| Q1-8. Satisfaction with treatment method | <0.001 | 2.20 | (1.43–3.38) |
| Q1-9. Atmosphere conducive to asking questions | <0.001 | 2.50 | (1.56–4.01) |
| Q2. Talking with physician about symptoms and treatments related to urination at least once every 10 visits | 0.23 | 1.44 | (0.79–2.63) |
| Age (≥70 years old) | 0.75 | 0.94 | (0.63–1.40) |
| Sex (female) | 0.44 | 1.17 | (0.78–1.76) |
| Duration of medication exposure is ≥3 months | 0.20 | 0.75 | (0.49–1.16) |
| Have not switched to another type of overactive bladder medication since starting to take it | 0.045 | 1.44 | (1.01–2.05) |
| Explanatory Variables | p-Value | OR | 95% CI |
|---|---|---|---|
| Q1-3. Symptom enquiry | <0.001 | 2.45 | (1.62–3.70) |
| Q1-4. Explanation of treatment method | 0.18 | 1.34 | (0.87–2.06) |
| Q1-5. Explanation of effects | 0.70 | 0.92 | (0.60–1.41) |
| Q1-6. Explanation of side effects | 0.80 | 0.96 | (0.68–1.34) |
| Q1-7. Explanation of treatment options and consultation | 0.42 | 0.87 | (0.63–1.21) |
| Q1-8. Satisfaction with treatment method | <0.001 | 1.97 | (1.36–2.85) |
| Q1-9. Atmosphere conducive to asking questions | 0.74 | 0.94 | (0.63–1.40) |
| Q2. Talking with physician about symptoms and treatments related to urination at least once every 10 visits. | 0.47 | 0.84 | (0.52–1.35) |
| Age (≥70 years old) | 0.86 | 1.03 | (0.75–1.40) |
| Sex (female) | <0.001 | 1.89 | (1.38–2.58) |
| Duration of medication exposure is ≥3 months. | 0.06 | 1.38 | (0.99–1.92) |
| Have not switched to another type of overactive bladder medication since starting to take it. | 0.002 | 1.53 | (1.16–2.01) |
| Association with Medical Care Satisfaction (Endpoint 1) | Association with Effectiveness of OAB Medication * (Endpoint 2) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Discontinuation Group | Continuation Group | Discontinuation Group | Continuation Group | |||||||||
| Explanatory Variables | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | Adjusted OR | 95% CI |
| Q1-1. Medication’s effectiveness | <0.001 | 4.22 | (2.00–8.92) | <0.001 | 8.43 | (5.16–13.78) | - | - | - | - | - | - |
| Q1-2. Medication’s side effects | 0.04 | 0.44 | (0.20–0.97) | <0.001 | 0.34 | (0.19–0.59) | - | - | - | - | - | - |
| Q1-3. Symptom enquiry | 0.11 | 0.41 | (0.14–1.21) | 0.64 | 1.18 | (0.59–2.36) | 0.97 | 1.02 | (0.42–2.43) | 0.001 | 2.59 | (1.46–4.61) |
| Q1-4. Explanation of treatment method | 0.08 | 2.98 | (0.88–10.07) | 0.85 | 0.93 | (0.47–1.85) | 0.20 | 1.91 | (0.71–5.15) | 0.17 | 1.50 | (0.84–2.67) |
| Q1-5. Explanation of effects | 0.67 | 0.78 | (0.25–2.43) | 0.11 | 1.71 | (0.88–3.32) | 0.27 | 0.58 | (0.22–1.53) | 0.92 | 0.97 | (0.55–1.72) |
| Q1-6. Explanation of side effects | 0.006 | 3.47 | (1.43–8.40) | 0.08 | 1.65 | (0.94–2.89) | 0.78 | 1.12 | (0.50–2.49) | 0.86 | 1.04 | (0.67–1.63) |
| Q1-7. Explanation of treatment options and consultation | 0.09 | 2.12 | (0.89–5.05) | 0.38 | 1.27 | (0.74–2.20) | 0.32 | 1.47 | (0.69–3.12) | 0.21 | 0.75 | (0.48–1.18) |
| Q1-8. Satisfaction with treatment method | 0.86 | 1.08 | (0.45–2.62) | <0.001 | 2.81 | (1.55–5.09) | 0.31 | 1.47 | (0.70–3.09) | 0.004 | 2.16 | (1.28–3.64) |
| Q1-9. Atmosphere conducive to asking questions | 0.08 | 2.57 | (0.90–7.35) | 0.01 | 2.32 | (1.19–4.54) | 0.77 | 1.14 | (0.49–2.65) | 0.14 | 0.65 | (0.36–1.16) |
| Q2. Talking with physician about symptoms and treatments related to urination at least once every 10 visits | 0.32 | 2.15 | (0.48–9.65) | 0.20 | 1.76 | (0.74–4.18) | 0.61 | 0.78 | (0.30–2.03) | 0.61 | 0.83 | (0.41–1.69) |
| Age (≥70 years old) | 0.26 | 0.61 | (0.26–1.44) | 0.31 | 1.33 | (0.77–2.32) | 0.76 | 1.12 | (0.53–2.37) | 0.68 | 1.09 | (0.72–1.65) |
| Sex (female) | 0.88 | 0.94 | (0.40–2.22) | 0.23 | 1.42 | (0.81–2.50) | 0.22 | 1.58 | (0.76–3.27) | 0.002 | 1.94 | (1.27–2.95) |
| Duration of medication exposure is ≥3 months | 0.11 | 2.07 | (0.86–5.00) | 0.07 | 0.53 | (0.26–1.06) | 0.32 | 1.45 | (0.69–3.03) | 0.002 | 2.30 | (1.36–3.87) |
| Have not switched to another type of overactive bladder medication since starting to take it | 0.48 | 1.31 | (0.62–2.76) | 0.04 | 1.65 | (1.03–2.65) | 0.63 | 0.86 | (0.46–1.60) | 0.006 | 1.65 | (1.16–2.36) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izumi, N.; Matsuo, T.; Matsukawa, Y. Associations among Physician–Patient Communication, Patient Satisfaction, and Clinical Effectiveness of Overactive Bladder Medication: A Survey of Patients with Overactive Bladder. J. Clin. Med. 2022, 11, 4087. https://doi.org/10.3390/jcm11144087
Izumi N, Matsuo T, Matsukawa Y. Associations among Physician–Patient Communication, Patient Satisfaction, and Clinical Effectiveness of Overactive Bladder Medication: A Survey of Patients with Overactive Bladder. Journal of Clinical Medicine. 2022; 11(14):4087. https://doi.org/10.3390/jcm11144087
Chicago/Turabian StyleIzumi, Naoko, Tomohiro Matsuo, and Yoshihisa Matsukawa. 2022. "Associations among Physician–Patient Communication, Patient Satisfaction, and Clinical Effectiveness of Overactive Bladder Medication: A Survey of Patients with Overactive Bladder" Journal of Clinical Medicine 11, no. 14: 4087. https://doi.org/10.3390/jcm11144087