Health has been a long-term target of the World Health Organization (WHO) and United Nations (UN), where the meaning of health is sometimes restricted to longevity without diseases. However, health is perceived differently by the wider population, and thus should be reconsidered to realize Universal Health Coverage (UHC), which is one of the most important targets of the Sustainable Development Goals (SDGs). Based on health from the perspective of medical anthropology and historical changes since ancient China and global diversity, we propose a comprehensive framework for health impairments and how to tackle them. This framework may contribute to understanding health and realizing UHC in its true sense.
Health is a frequently used word in seeking well-being in the UN, through the changing approaches by World Health, International Health, Global Health, and Planetary Health (Horton et al. 2014).1 Simultaneously, health equity has become the target for Universal Health Coverage (UHC). Sustainable development goals (SDGs) include “Ensure healthy lives and promote well-being for all at all ages” as the third goal.2
However, the meaning of “health” is sometimes restricted to longevity without diseases when medical professionals refer to UHC. Most professionals seem to believe that health can be achieved through medical and hygienic improvement, although the health concept has been defined as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” by the WHO.3 It is clear that health is not a natural existence, but an artificial concept. The authors have conducted long term research on the relationship between humans and the environment in rural areas of developing countries. When one of the authors asked the people in the Solomon Islands about the meaning of health, they replied that they learned about health in school education, but originally they did not have the concept of health in their traditional life. We need to reconsider the concept of health itself in a global context.
Universal health coverage (UHC) is one of the top targets of the SDGs. In developing countries, not only financial support with public insurance, but also geographically well-arranged and fully equipped medical facilities are needed. In some developed countries like the United States, large socioeconomic gaps cause financial difficulty and hinder access to medical facilities by poor and vulnerable people. Japan has established a medical treatment system that has mostly achieved UHC. It has achieved this by properly arranged medical facilities for all patients and various health insurance systems covering virtually all citizens.4 However, such “medical treatment for all” is still not enough from the viewpoint of public health. It functioned well under the pre-health transition periods, but does not always function well under the situation where the major cause of death is mainly by non-communicable diseases. Most non-communicable diseases have a longer duration of “in-disease” status than communicable diseases, which may result in a higher cost of treatment and maintenance. Since some diseases cannot be completely cured, but kept in remission, care and checkups for prevention of recrudescence are needed.
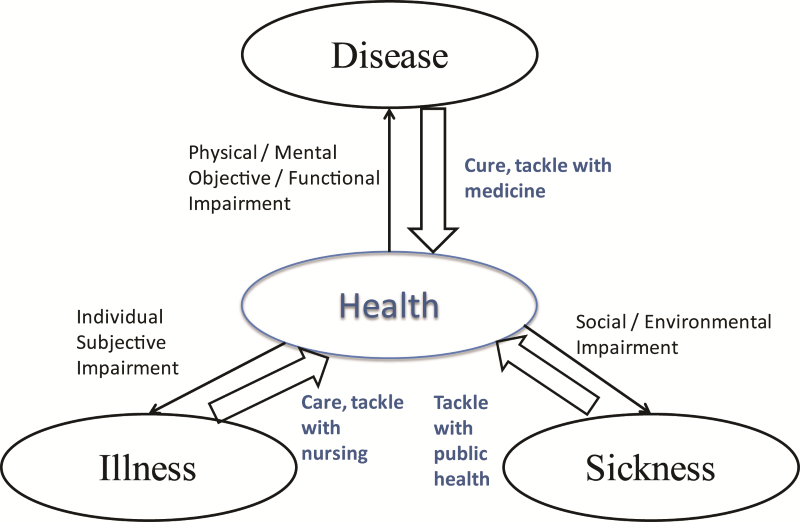
Health itself is a complicated concept. It varies by culture and social contexts.5 Therefore, this short manuscript focuses on suggesting the overview about how to tackle health impairments for an integrative view on health. This is necessary for promoting worldwide UHC. Many textbooks on medical anthropology classify the types of health impairments into disease, illness and sickness: disease is objective, measurable, functional impairment of health, which should be universally common, and can be classified by the global standard (International Classification of Diseases; ICD): illness is subjective impairment of health, which is not always caused by diseases; sickness is sometimes used as a rough concept, including disease and illness, but also the state regarded as being unable to play the complete role of a healthy person in the society,5,6 in other words: social impairment of health.
There are three different ways of tackling health impairments: recovery from disease is “curing”, which is mainly done through medical treatment; recovery from illness is “care”, which is a major purpose of nursing; and recovery from sickness is “well-being”, including social environment, which is the major purpose of public health. Based on these considerations, we propose a framework to integrate these health impairments and how to tackle them (Figure 1). To realize UHC, these multi-aspects of health should be addressed as a whole. Some activities related to UHC only focus on financial support for medical treatment. Other activities related to UHC only focus on providing appropriate medical treatment for the patients, but prevention and socioenvironmental improvement are sometimes forgotten or left behind. This framework may contribute to reminding ourselves of the importance of health as a whole.

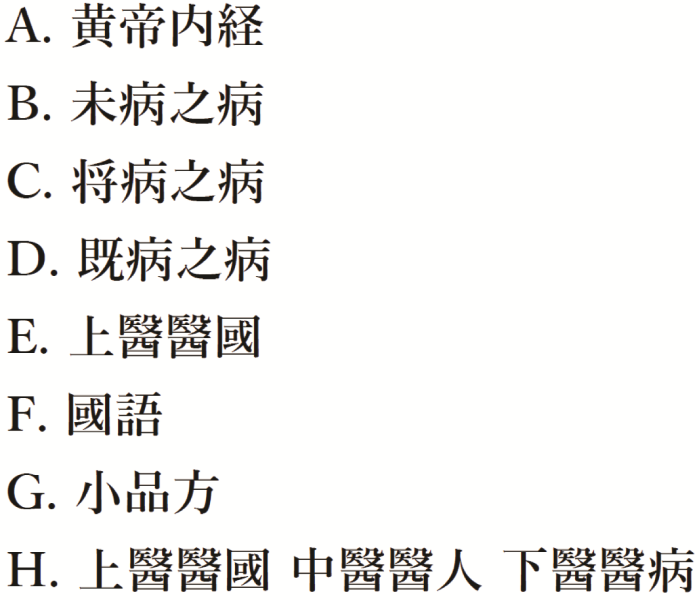
The Ancient Chinese may have known this. The oldest Chinese medical textbook “Huang Dee: Nai-Ching (Figure 2; a)” described the evaluation of doctors as “Superior doctors treat the disease before getting it (Figure 2; b), mediocre doctors treat the disease on time just getting it (Figure 2; c), inferior doctors treat the already full blown disease (Figure 2; d)”.7 Probably combining this description with “Superior doctors heal the nation (Figure 2; e)” in “Guoyu (Figure 2; f)”, "Xiao Pin Fang (Figure 2; g)" in the 5th Century seemed to describe the classification of doctors as, “The superior doctor heals the nation, the middle doctor deals with the person, the inferior doctor treats the disease (Figure 2; h)”.8 Later in the 7th Century, it is referred to anonymously in the famous medical textbook (Sun 652)9 and the original “Xiao Ping Fang” has been lost, so that the phrase is well known, but the origin is vague. From our viewpoint, this maxim may be rephrased as “the roles of the superior, middle, and inferior doctors correspond to public health, nursing and medicine”. Obviously these are interrelated, but the major purposes differ; subsequently, the approaches must differ. Therefore, education and/or human resource development system should differ. The WHO is already aware of the importance of peace, shelter, social justice and equity for health as a “prerequisite”. Its awareness is shown in the Ottawa Charter,10 which stresses the need to prevent illness or sickness rather than disease. It is also needed to realize UHC.

Acknowledgements: The authors appreciate Mr. Scott Lucas (Nagasaki University) for his contribution on the English side.
Competing interests: The authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no conflict of interest.
Correspondence to:
Minato Nakazawa, PhD
Kobe University, Graduate School of Health Sciences,
Suma-ku,Tomogaoka 7-10-2, Kobe 654-0142, Japan
[email protected]