Safety Evaluation of Tadalafil Treatment for Fetuses with Early-Onset Growth Restriction (TADAFER): Results from the Phase II Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Trial Design and Study Population
2.2. Randomization
2.3. Safety Evaluation
2.4. Other Evaluation
2.5. Criteria for Delivery
2.6. Statistical Analysis
2.7. Funding
2.8. Participant and Public Involvement
3. Results
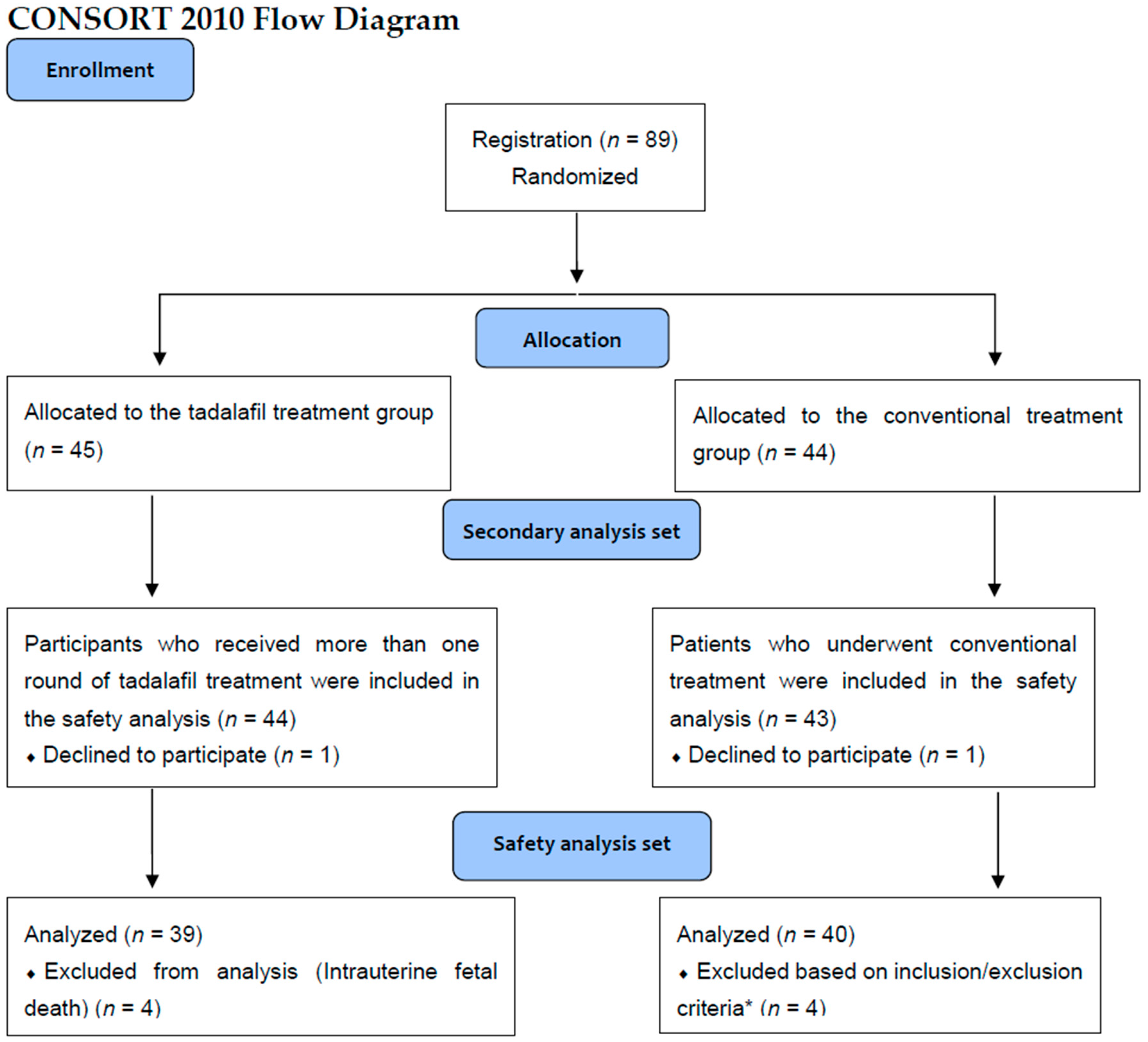
3.1. Study Profile
3.2. Adverse Events
3.3. Other Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thornton, J.G.; Hornbuckle, J.; Vail, A.; Spiegelhalter, D.J.; Levene, M.; GRIT Study Group. Infant wellbeing at 2 years of age in the Growth Restriction Intervention Trial (GRIT): Multicentred randomised controlled trial. Lancet 2004, 364, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Nardozza, L.M.; Araujo Júnior, E.; Barbosa, M.M.; Caetano, A.C.; Lee, D.J.; Moron, A.F. Fetal growth restriction: Current knowledge to the general Obs/Gyn. Arch. Gynecol. Obstet. 2012, 286, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hui, L.; Challis, D. Diagnosis and management of fetal growth restriction: The role of fetal therapy. Best Pract. Res. Clin. Obstet. Gynaecol. 2008, 22, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Meher, S.; Duley, L.; Hunter, K.; Askie, L. Antiplatelet therapy before or after 16 weeks’ gestation for preventing preeclampsia: An individual participant data meta-analysis. Am. J. Obstet. Gynecol. 2017, 216, 121.e2–128.e2. [Google Scholar] [CrossRef]
- Dodd, J.M.; McLeod, A.; Windrim, R.C.; Kingdom, J. Antithrombotic therapy for improving maternal or infant health outcomes in women considered at risk of placental dysfunction. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Roberge, S.; Nicolaides, K.; Demers, S.; Hyett, J.; Chaillet, N.; Bujold, E. The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: Systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2017, 216, 110–120.e6. [Google Scholar] [CrossRef]
- Costantine, M.M.; Cleary, K.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Obstetric—Fetal Pharmacology Research Units Network. Pravastatin for the prevention of preeclampsia in high-risk pregnant women. Obstet. Gynecol. 2013, 121, 349–353. [Google Scholar] [CrossRef]
- Von Dadelszen, P.; Dwinnell, S.; Magee, L.A.; Carleton, B.C.; Gruslin, A.; Lee, B.; Lim, K.I.; Liston, R.M.; Miller, S.P.; Rurak, D.; et al. Sildenafil citrate therapy for severe early-onset intrauterine growth restriction. BJOG 2011, 118, 624–628. [Google Scholar] [CrossRef]
- Samangaya, R.A.; Mires, G.; Shennan, A.; Skillern, L.; Howe, D.; McLeod, A.; Baker, P.N. A randomised, double-blinded, placebo-controlled study of the phosphodiesterase type 5 inhibitor sildenafil for the treatment of preeclampsia. Hypertens Pregnancy 2009, 28, 369–382. [Google Scholar] [CrossRef]
- Sharp, A.; Conforth, C.; Jackson, R.; Harrold, J.; Turner, M.A.; Kenny, L.C.; Baker, P.N.; Johnstone, E.D.; Khalil, A.; von Dadelszen, P.; et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): A multicenter, randomized, placebo-controlled, double-blind trial. Lancet Child. Adolesc. Health 2018, 2, 93–102. [Google Scholar] [CrossRef]
- Dastjerdi, M.V.; Hosseini, S.; Bayani, L. Sildenafil citrate and uteroplacental perfusion in fetal growth restriction. J. Res. Med. Sci. 2012, 17, 632–636. [Google Scholar] [PubMed]
- Yoshikawa, K.; Umekawa, T.; Maki, S.; Kubo, M.; Nii, M.; Tanaka, K.; Tanaka, H.; Osato, K.; Kamimoto, Y.; Kondo, E.; et al. Tadalafil improves L-NG-nitroarginine methyl ester-induced preeclampsia with fetal growth restriction-like symptoms in pregnant mice. Am. J. Hypertens 2017, 31, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, R.; Umekawa, T.; Yoshikawa, K.; Owa, T.; Magawa, S.; Furuhashi, F.; Tsuji, M.; Maki, S.; Shimada, K.; Kaneda, M.K.; et al. Tadalafil treatment in mice for preeclampsia with fetal growth restriction has neuro-benefic effects in offspring through modulating prenatal hypoxic conditions. Sci. Rep. 2019, 9, 234. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Umekawa, T.; Maekawa, Y.; Tanaka, H.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Ikeda, T. Retrospective study of tadalafil for fetal growth restriction:Impact on maternal and perinatal outcomes. J. Obstet. Gynaecol. Res. 2017, 43, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Tanaka, H.; Maki, S.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Umekawa, T.; Kondo, E.; Ikeda, T. Safety and dose-finding trial of tadalafil administered for fetal growth restriction: A phase-1 clinical study. J. Obstet. Gynaecol. Res. 2017, 43, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.L.; Loose, J.M.; Jenkin, G.; Wallace, E.M. The effects of sildenafil citrate (Viagra) on uterine blood flow and well being in the intrauterine growth-restricted fetus. Am. J. Obstet. Gynecol. 2009, 200, 102.e1–102.e7. [Google Scholar] [CrossRef] [PubMed]
- Nassar, A.H.; Masrouha, K.Z.; Itani, H.; Nader, K.A.; Usta, I.M. Effects of sildenafil in Nω-nitro-L-arginine methyl ester-induced intrauterine growth restriction in a rat model. Am. J. Perinatol. 2012, 29, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Satterfield, M.C.; Bazer, F.W.; Spencer, T.E.; Wu, G. Sildenafil citrate treatment enhances amino acid availability in the conceptus and fetal growth in an ovine model of intrauterine growth restriction. J. Nutr. 2010, 140, 251–258. [Google Scholar] [CrossRef]
- Oyston, C.; Stanley, J.L.; Oliver, M.H.; Bloomfield, F.H.; Baker, P.N. Maternal administration of sildenafil citrate alters fetal and placental growth and fetal-placental vascular resistance in the growth-restricted ovine fetus. Hypertension 2016, 68, 760–767. [Google Scholar] [CrossRef]
- Stanley, J.L.; Andersson, I.J.; Oliver, M.H.; Bloomfield, F.H.; Baker, P.N. Sildenafil citrate rescues fetal growth in the catechol-O-methyl transferase knockout mouse model. Hypertension 2012, 59, 1021–1028. [Google Scholar] [CrossRef]
- Dilworth, M.R.; Andersson, I.; Renshall, L.J.; Cowley, E.; Baker, P.; Greenwood, S.; Sibley, C.P.; Wareing, M. Sildenafil citrate increases fetal weight in a mouse model of fetal growth restriction with a normal vascular phenotype. PLoS ONE 2013, 8, e77748. [Google Scholar] [CrossRef] [PubMed]
- Kanasaki, K.; Palmsten, K.; Sugimoto, H.; Ahmad, S.; Hamano, Y.; Xie, L.; Parry, S.; Augustin, H.G.; Gattone, V.H.; Folkman, J.; et al. Deficiency in catechol-O-methyltransferase and 2-methoxyoestradiol is associated with pre-eclampsia. Nature 2008, 453, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Groom, K.; McCowan, L.; Mackay, L.K.; Lee, A.C.; Gardener, G.; Unterscheider, J.; Sekar, R.; Dickinson, J.E.; Muller, P.; Reid, R.A.; et al. STRIDER NZAus: A multicentre randomised controlled trial of sildenafil therapy in early-onset fetal growth restriction. BJOG 2019. [Google Scholar] [CrossRef] [PubMed]
- Groom, K.; Ganzevoot, W.; Alfirevic, Z.; Lim, K.; Papageorghiou, A.T.; STRIDER Consortium. Clinicians should stop prescribing sildenafil for fetal growth restriction (FGR): Comment from the STRIDER Consortium. Ultrasound Obstet. Gynecol. 2018, 52, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Umekawa, T.; Maki, S.; Kubo, M.; Tanaka, H.; Nii, M.; Tanaka, K.; Osato, K.; Kamimoto, Y.; Tamaru, S.; Ogura, T.; et al. TADAFER II: Tadalafil treatment for fetal growth restriction—A study protocol for a multicenter randomized controlled phase II trial. BMJ Open 2018, 8, e020948. [Google Scholar] [CrossRef]
- Minakami, H.; Maeda, T.; Fujii, T.; Hamada, H.; Iitsuka, Y.; Itakura, A.; Itoh, H.; Iwashita, M.; Kanagawa, T.; Kanai, M.; et al. Guidelines for obstetrical practice in Japan:Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J. Obstet. Gynaecol. Res. 2014, 40, 1469–1499. [Google Scholar] [CrossRef]
- Kusuda, S.; Fujimura, M.; Sakuma, I.; Aotani, H.; Kabe, K.; Itani, Y.; Ichiba, H.; Matsunami, K.; Nishida, H.; Neonatal Research Network, Japan. Morbidity and mortality of infants with very low birth weight in Japan: Center variation. Pediatrics 2006, 118, e1130–e1138. [Google Scholar] [CrossRef]
- Walton, R.B.; Reed, L.C.; Estrada, S.M.; Schmiedecke, S.S.; Villazana-Kretzer, D.L.; Napolitano, P.G.; Ieronimakis, N. Evaluation of sildenafil and tadalafil for reversing constriction of fetal arteries in a human placenta perfusion model. Hypertension 2018, 72, 167–176. [Google Scholar] [CrossRef]
- Costeloe, K.L.; Hennessy, E.M.; Haider, S.; Stacey, F.; Marlow, N.; Draper, E.S. Short term outcomes after extreme preterm birth in England: Comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ 2012, 345, e7976. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
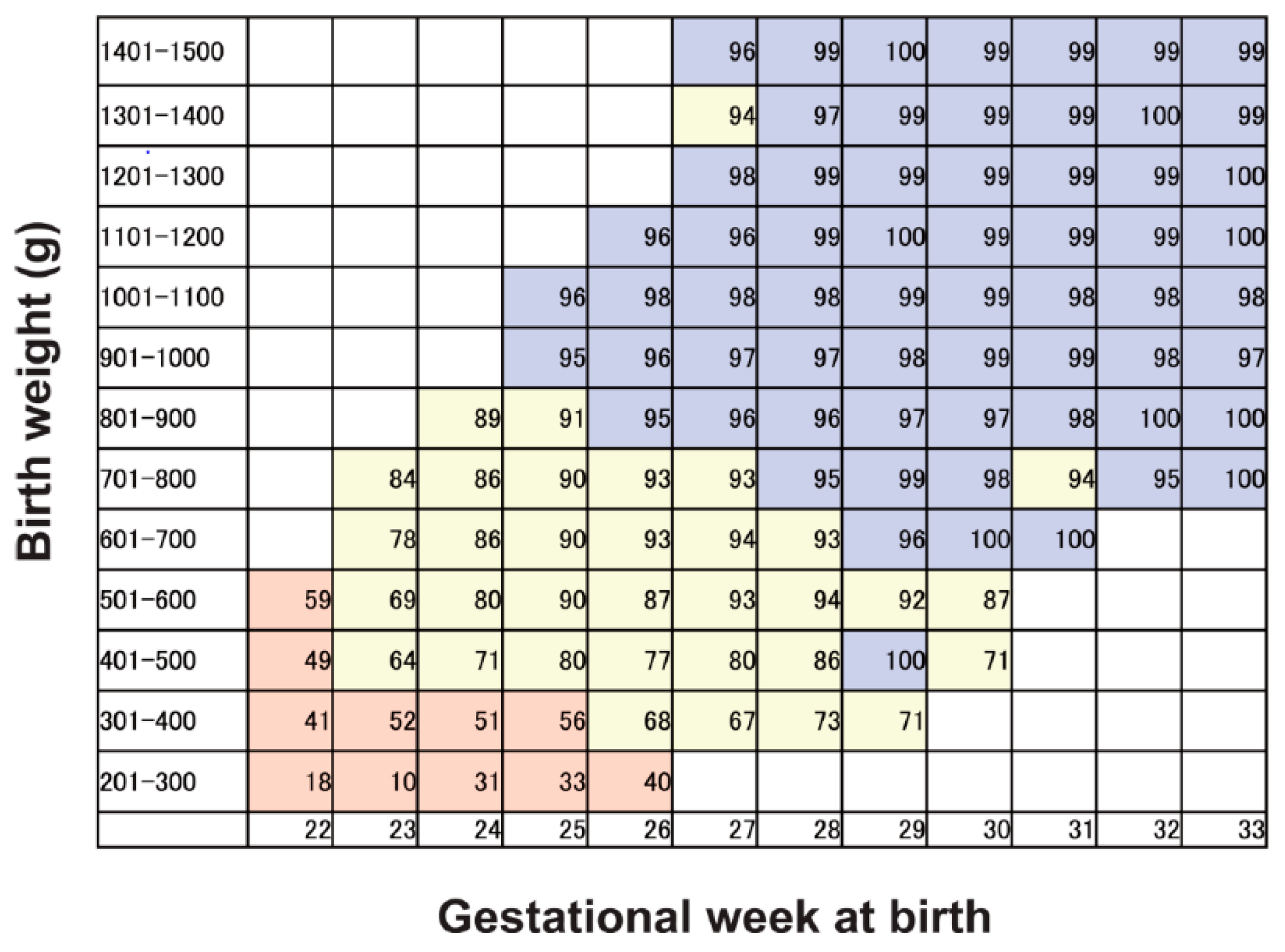
| Infant Survival Rate in the Neonatal Intensive Care Unit (NICU) (See Figure 1) | Fetal Indication for Delivery |
|---|---|
| Zone 1 | Decide timing of delivery depending on available therapeutic measures at the NICU in each institute. |
| Zone 2 | Consider delivery if at least one of three findings is made. 1. Reversed umbilical artery blood flow during diastole. 2. Score less than 4 on the fetal biophysical profile score. 3. Fetal heart rate patterns in the orange or red category for more than 30 min. |
| Zone 3 | Consider delivery if at least one of the following five findings is made. 1. Reversed or absent umbilical artery blood flow during diastole, 2. Score less than 4 on the fetal biophysical profile score (score less than 6 on the fetal biophysical profile score if oligohydramnios is present). 3. Fetal heart rate patterns in the orange or red category for more than 30 min. 4. Positive contraction stress test. 5. Impaired fetal head circumference growth for more than 2 weeks, |
| Tadalafil Treatment Group | Conventional Treatment Group | |||
|---|---|---|---|---|
| Safety Analysis Set | Secondary Analysis Set | Safety Analysis Set | Secondary Analysis Set | |
| (n = 44) | (n = 40) | (n = 43) | (n = 39) | |
| Age (years) | 34 (21–44) | 33 (27–38) | 34 (20–43) | 34 (29–37) |
| Height (cm) | 158 (147–170) | 157 (153–160) | 156 (144–168) | 158 (155–162) |
| Weight (kg) | 56 (45–91) | 56 (52–64) | 56 (44–75) | 57 (51–61) |
| Smoking history | 3 (7%) | 3 (8%) | 2 (5%) | 2 (5%) |
| Nulliparous | 21 (47%) | 22 (55%) | 26 (60%) | 15 (38%) |
| Gestational age at registration (weeks) | 29 (25–32) | 28 (25–32) | 28 (24.5–31) | 29 (26–32) |
| Obstetrics complications | ||||
| Gestational hypertension | 6 (13%) | 6 (15%) | 5 (12%) | 3 (8%) |
| Preeclampsia | 3 (7%) | 1 (3%) | 3 (7%) | 3 (8%) |
| Gestational diabetes | 5 (11%) | 5 (13%) | 0 (0%) | 0 (0%) |
| Ultrasound sonographic finding | ||||
| Estimated fetal body weight (g) | 887 (444–1349) | 887 (520–1361) | 809 (504–1348) | 900 (620–1384) |
| Standard deviation of estimated fetal body weight | −2.3 (−2.8 to −1.9) | −2.3 (−2.8 to −2.0) | −2.2 (−2.9 to −2.0) | −2.1 (−2.6 to −1.9) |
| Percentile of estimated fetal body weight | 2.1 (0.3–2.2) | 2.1 (0.3–2.2) | 2.2 (0.2–2.3) | 2.2 (0.2–2.3) |
| Umbilical artery Doppler abnormal *1 | 2 (5%) | 2(5%) | 3 (7%) | 0 (0%) |
| Uterine artery Doppler abnormal *2 | 12 (27%) | 10(30%) | 15 (35%) | 11 (32%) |
| Maternal factors | ||||
| Systolic BP (mmHg) | 120 (88–151) | 114 (103–130) | 114 (90–185) | 120 (106–132) |
| Diastolic BP (mmHg) | 73 (46–100) | 71 (59–81) | 71 (49–110) | 73 (65–80) |
| Creatinine (mg/dL) | 0.48 (0.31–0.9) | 0.47(0·41–0·53) | 0.47 (0.34–0.74) | 0.47(0.40–0.53) |
| AST (IU/L) | 17 (9–49) | 16 (14–21) | 16 (10–31) | 16 (13–21) |
| ALT (IU/L) | 11 (4–71) | 12 (8–17) | 12 (5–49) | 11 (7–15) |
| Albumin (g/dL) | 3.2 (2.2–4) | 3.3 (3.0–3.5) | 3.3 (2.1–4.0) | 3.2 (3.0–3.5) |
| Platelet count (×104/μL) | 24 (9–35) | 25.0 (22.2–28.1) | 24 (9–37) | 23.2 (19.4–26.2) |
| Tadalafil Treatment Group (n = 44) | Conventional Treatment Group (n = 43) | p Value | |
|---|---|---|---|
| Intrauterine fetal death | 0 (0%) | 4 (9%) | NA |
| Perinatal mortality | 0 (0%) | 5 (12%) | NA |
| Neonatal death | 1 (2%) | 1 (3%) | >0.99 |
| Infant death (6 months after stopping trial) | 0 (0%) | 2 (4%) | NA |
| Total death | 1 (2%) | 7 (16%) | 0.03 |
| Timing of Death | Allocation | Gestational Weeks at Registration | Gestational Weeks at Delivery | Treatment Period (Days) | Birth Weight (g) | Age in Days at the Time of Death (Days) | Cause of Death | Umbilical Artery Flow Absent or Reverse at Registration |
|---|---|---|---|---|---|---|---|---|
| Fetal death | Conventional treatment | 23 | 25 | 10 | 328 | NA | Placental abruption | + |
| Fetal death | Conventional treatment | 20 | 20 | 4 | <300 | NA | Unknown | + |
| Fetal death | Conventional treatment | 25 | 25 | 6 | 440 | NA | Unknown | + |
| Fetal death | Conventional treatment | 21 | 25 | 30 | 484 | NA | Unknown | − |
| Neonatal death | Tadalafil treatment | 21 | 23 | 16 | 317 | 17 | Necrotizing enterocolitis, Sepsis | − |
| Neonatal death | Conventional treatment | 24 | 25 | 7 | 440 | 0 | Respiratory failure | − |
| Infant death | Conventional treatment | 27 | 27 | 0 | 704 | 98 | Sepsis, Renal failure | − |
| Infant death | Conventional treatment | 28 | 32 | 25 | 730 | 167 | Necrotizing enterocolitis | − |
| Tadalafil Treatment Group (n = 44) | Conventional Treatment Group (n = 43) | Relative Risk | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|---|
| Infant admitted to NICU | 36 (82%) | 33 (77%) | 1.03 | 0.84–1.27 | 0.61 |
| Oxygen dependency | 16 (36%) | 18 (42%) | 0.82 | 0.49–1.37 | 0.66 |
| Necrotizing enterocolitis | 1 (2%) | 2 (5%) | 0.48 | 0.04–5.19 | 0.62 |
| Retinopathy of prematurity | 5 (11%) | 4 (9%) | 1.22 | 0.35–4.24 | >0.99 |
| Intraventricular hemorrhage | 0 (0%) | 1 (2%) | NA | NA | 0.49 |
| Periventricular leukomalacia | 1 (2%) | 0 (0%) | NA | NA | >0.99 |
| Hypoxic ischemic encephalopathy | 0 (0%) | 0 (0%) | NA | NA | >0.99 |
| Respiratory distress syndrome | 9 (20%) | 12 (28%) | 0.67 | 0.32–1.41 | 0.46 |
| Surfactant use | 7 (16%) | 11 (26%) | 0.57 | 0.24–1.31 | 0.30 |
| Chronic pulmonary disease | 6 (14%) | 3 (7%) | 1.94 | 0.52–7.32 | 0.48 |
| Persistent pulmonary hypertension of the newborn | 2 (5%) | 2 (5%) | 0.97 | 0.14–6.62 | >0.99 |
| Patent ductus arteriosus | 5 (11%) | 5 (12%) | 0.97 | 0.30–3.13 | >0.99 |
| Anemia of prematurity | 12 (27%) | 15 (35%) | 0.73 | 0.39–1.36 | 0.49 |
| Meconium plug syndrome | 2(5%) | 0(0%) | NA | NA | 0.49 |
| Tadalafil Treatment Group (n = 44) | Conventional Treatment Group (n = 43) | |||||||
|---|---|---|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
| Headache | 25(57%) | 1 (2%) | 0 (0%) | 0 (0%) | 11 (26%) | 0(0%) | 0 (0%) | 1 (2%) |
| Facial flushing | 16 (36%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Palpitations | 5 (11%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (5%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Anorexia | 9 (20%) | 1 (2%) | 0 (0%) | 0 (0%) | 3 (7%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Nausea | 8 (18%) | 1 (2%) | 0 (0%) | 0 (0%) | 3 (7%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Dizziness | 6 (14%) | 1 (2%) | 0 (0%) | 0 (0%) | 2 (5%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Muscle pain | 5 (11%) | 1 (2%) | 0 (0%) | 0 (0%) | 3 (7%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Nasal hemorrhage | 7 (16%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Indigestion | 1 (2%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (2%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Diarrhea | 3 (7%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (5%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Breathing trouble | 5 (11%) | 0 (0%) | 0 (0%) | 0 (0%) | 4 (9%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Tadalafil Treatment Group (n = 40) | Conventional Treatment Group (n = 39) | p-Value | |
|---|---|---|---|
| Fetal growth velocity (g/day) | 14.5 (7.3) | 12.9 (8.2) | 0.37 |
| Tadalafil Treatment Group (n = 40) | Conventional Treatment Group (n = 39) | p Value | |
|---|---|---|---|
| Prolongation of GA (days) | 47.2 (27.2) | 37.9 (24.1) | 0.11 |
| GA at birth (weeks) | 37.0 (33.9–37.9) | 36.0 (31.0–37.6) | 0.23 |
| Birth weight (g) | 1639 (615) | 1548 (713) | 0.55 |
| Standard deviation of birth weight | −2.5 (−3.2 to −1.5) | −2.1 (−3.2 to −0.9) | 0.76 |
| Percentile of birth weight | 0.6 (0.1–6.1) | 1.8 (0.1–5.5) | 0.81 |
| Maximum vertical pocket (cm) | 4.3 (3.2–5.3) | 4.1 (3.2–5.2) | 0.93 |
| Onset of hypertensive disorders of pregnancy *, ** | |||
| 1 week from the start of treatment | 0 (0%) | 1 (3%) | >0.99 |
| 2 weeks from the start of treatment | 0 (0%) | 3 (9%) | 0.24 |
| 3 weeks from the start of treatment | 0 (0%) | 4 (13%) | 0.11 |
| 4 weeks from the start of treatment | 0 (0%) | 4 (13%) | 0.11 |
| >4 weeks from the start of treatment | 2 (7%) | 5 (16%) | 0.43 |
| Obstetric complication | |||
| Abruption of placenta | 2 (5%) | 1 (2%) | >0.99 |
| Gestational diabetes | 5 (11%) | 0 (0%) | 0.06 |
| Cesarean section | 29 (74%) | 31 (79%) | 0.79 |
| Newborn’s sex | |||
| Male | 17 (43%) | 18 (46%) | 0.82 |
| Female | 23 (58%) | 21 (54%) | 0.82 |
| Apgar score | |||
| 1 min | 8 (7–8) | 8 (5–8) | 0.76 |
| 5 min | 9 (9–9) | 9 (8–9) | 0.30 |
| Umbilical cord blood gas analysis | |||
| pH | 7.284 (7.245–7.327) | 7.288 (7.262–7.317) | 0.66 |
| BE | −4.3 (3.9) | −3.5 (3.6) | 0.35 |
| Intrauterine fetal death | 0 (0%) | 4 (9%) | 0.06 |
| Perinatal mortality | 0 (0%) | 4 (9%) | 0.06 |
| Neonatal death | 1 (3%) | 1 (3%) | >0.99 |
| Use of aspirin | 2 (5%) | 1 (3%) | >0.99 |
| Fetal growth velocity in the two weeks after the protocol-defined treatment (g/day) | 19.1 (9.5) | 14.3 (8.6) | 0.02 |
| Fetal growth rate in the two weeks after the protocol-defined treatment and from the first day of the protocol-defined treatment to birth (%/day) | 2.4 (1.0) | 1.8 (1.0) | 0.01 |
| Fetal growth rate from the first day of the protocol-defined treatment to birth (%/day) | 1.9 (1.1) | 1.5 (1.4) | 0.14 |
| Tadalafil Treatment Group (n = 40) | Conventional Treatment Group (n = 39) | p-Value | |
|---|---|---|---|
| Umbilical artery | |||
| PI at registration | 1.03 (0.95–1.28) | 1.14 (0.98–1.54) | 0.43 |
| MoM | 1.03 (0.85–1.19) | 1.09 (0.91–1.24) | 0.74 |
| PI 1 week from the start of treatment | 0.98 (0.86–1.29) | 1.09 (0.95–1.36) | 0.18 |
| MoM | 0.94 (0.84–1.14) | 1.09 (0.90–1.20) | 0.50 |
| PI 2 weeks from the start of treatment | 0.66 (0.61–0.72) | 0.66 (0.60–0.73) | 0.72 |
| MoM | 1.05 (0.90–1.22) | 1.01 (0.90–1.17) | 0.71 |
| PI 3 weeks from the start of treatment | 0.63 (0.54–0.72) | 0.64 (0.59–0.73) | 0.37 |
| MoM | 1.01 (0.81–1.17) | 1.01 (0.89–1.22) | 0.93 |
| Middle cerebral artery | |||
| PI at registration | 1.57 (1.28–1.96) | 1.54 (1.15–1.89) | 0.66 |
| MoM | 0.85 (0.70–1.05) | 0.80 (0.69–0.92) | 0.75 |
| PI 1 week from the start of treatment | 1.65 (1.37–2.06) | 1.68 (1.44–2.14) | 0.73 |
| MoM | 0.86 (0.77–1.06) | 0.89 (0.78–1.07) | 0.72 |
| PI 2 weeks from the start of treatment | 1.71 (1.29–1.85) | 1.61 (1.31–1.82) | 0.63 |
| MoM | 0.88 (0.71–0.98) | 0.85 (0.70–0.95) | 0.81 |
| PI 3 weeks from the start of treatment | 1.58 (1.48–1.98) | 1.66 (1.46–2.02) | 0.95 |
| MoM | 0.82 (0.74–1.01) | 0.88 (0.70–1.07) | 0.66 |
| Uterine artery | |||
| PI at registration | 1.04 (0.88–1.49) | 1.24 (0.80–1.82) | 0.23 |
| MoM | 1.38 (1.12–2.03) | 1.44 (1.16–1.92) | 0.57 |
| PI 1 week from the start of treatment | 0.96 (0.76–1.42) | 0.79 (0.70–1.24) | 0.28 |
| MoM | 1.20 (1.01–1.48) | 1.34 (1.04–1.97) | 0.36 |
| PI 2 weeks from the start of treatment | 1.06 (0.70–1.47) | 0.94 (0.73–1.35) | 0.69 |
| MoM | 1.35 (1.00–1.89) | 1.42 (1.08–1.86) | 0.35 |
| PI 3 weeks from the start of treatment | 0.94 (0.75–1.22) | 0.96 (0.62–1.55) | 0.96 |
| MoM | 1.15 (0.91–2.04) | 1.40 (1.14–1.78) | 0.75 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maki, S.; Tanaka, H.; Tsuji, M.; Furuhashi, F.; Magawa, S.; Kaneda, M.K.; Nii, M.; Tanaka, K.; Kondo, E.; Tamaru, S.; et al. Safety Evaluation of Tadalafil Treatment for Fetuses with Early-Onset Growth Restriction (TADAFER): Results from the Phase II Trial. J. Clin. Med. 2019, 8, 856. https://doi.org/10.3390/jcm8060856
Maki S, Tanaka H, Tsuji M, Furuhashi F, Magawa S, Kaneda MK, Nii M, Tanaka K, Kondo E, Tamaru S, et al. Safety Evaluation of Tadalafil Treatment for Fetuses with Early-Onset Growth Restriction (TADAFER): Results from the Phase II Trial. Journal of Clinical Medicine. 2019; 8(6):856. https://doi.org/10.3390/jcm8060856
Chicago/Turabian StyleMaki, Shintaro, Hiroaki Tanaka, Makoto Tsuji, Fumi Furuhashi, Shoichi Magawa, Michiko K. Kaneda, Masafumi Nii, Kayo Tanaka, Eiji Kondo, Satoshi Tamaru, and et al. 2019. "Safety Evaluation of Tadalafil Treatment for Fetuses with Early-Onset Growth Restriction (TADAFER): Results from the Phase II Trial" Journal of Clinical Medicine 8, no. 6: 856. https://doi.org/10.3390/jcm8060856