Evaluation of the Effect of Different Doses of Low Energy Shock Wave Therapy on the Erectile Function of Streptozotocin (STZ)-Induced Diabetic Rats

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
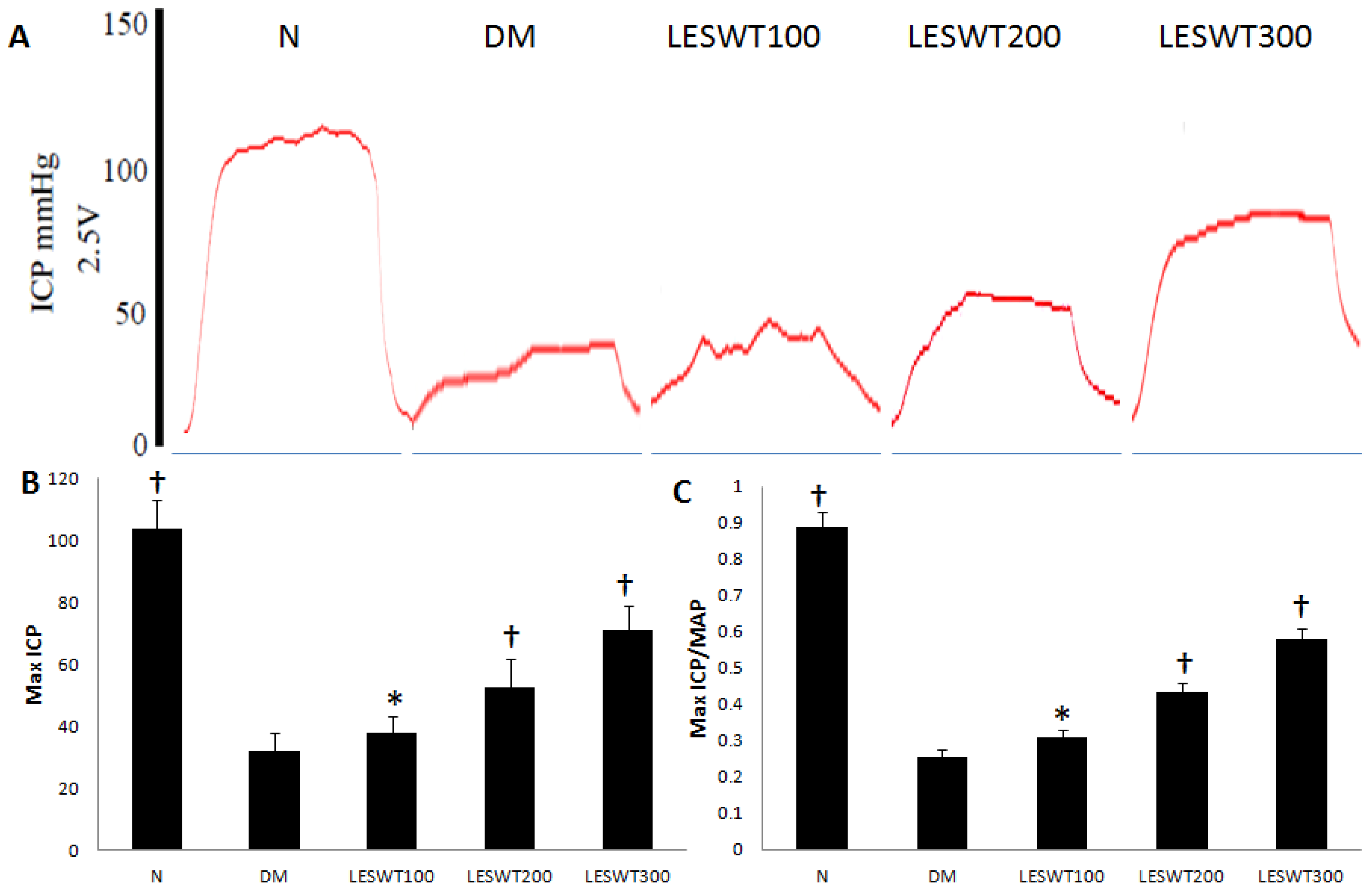
2.1. Effect of LESWT on Erectile Function
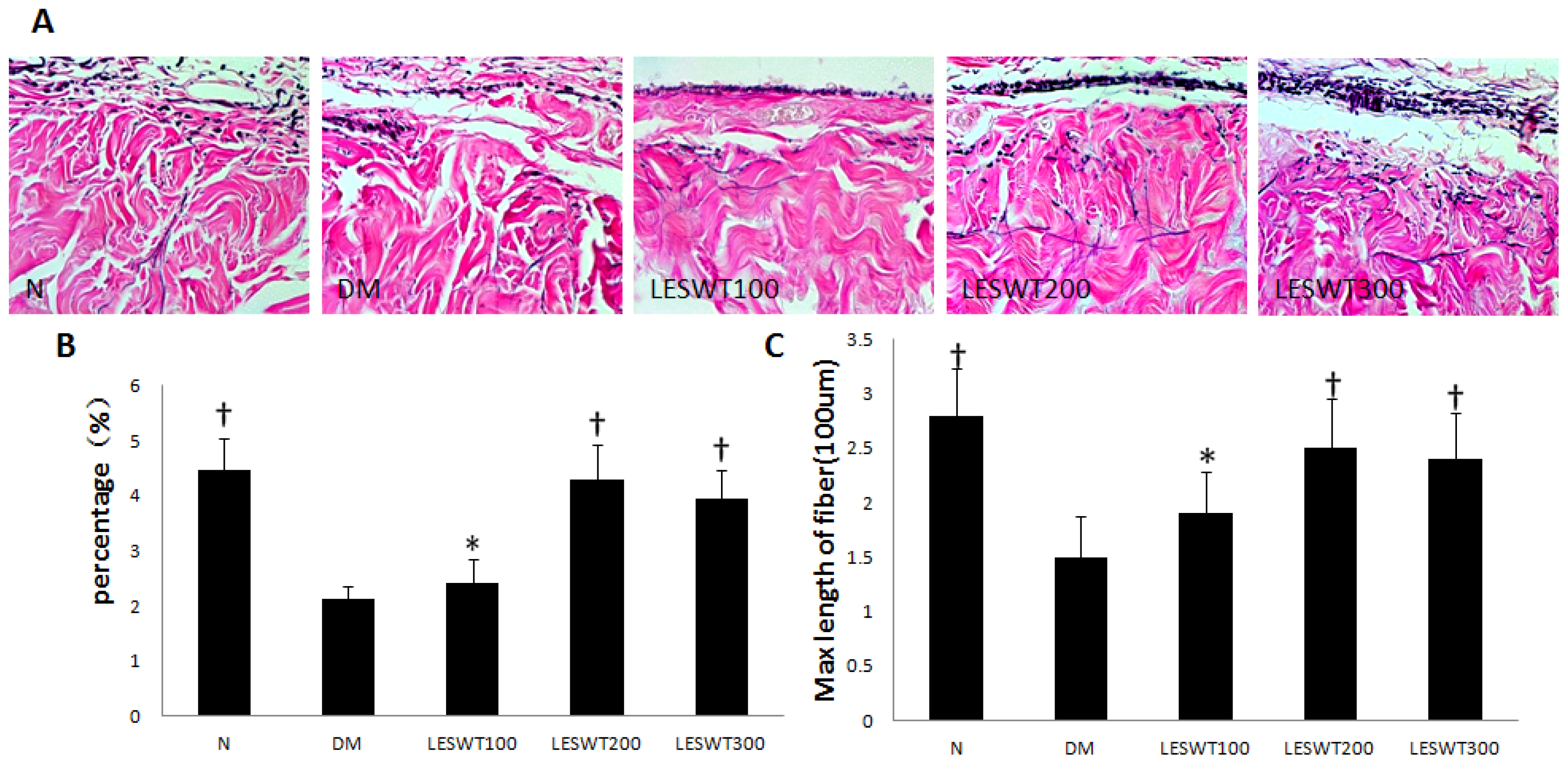
2.2. Effect of LESWT on Extracellular Matrix (ECM) in Corpus Cavernosum
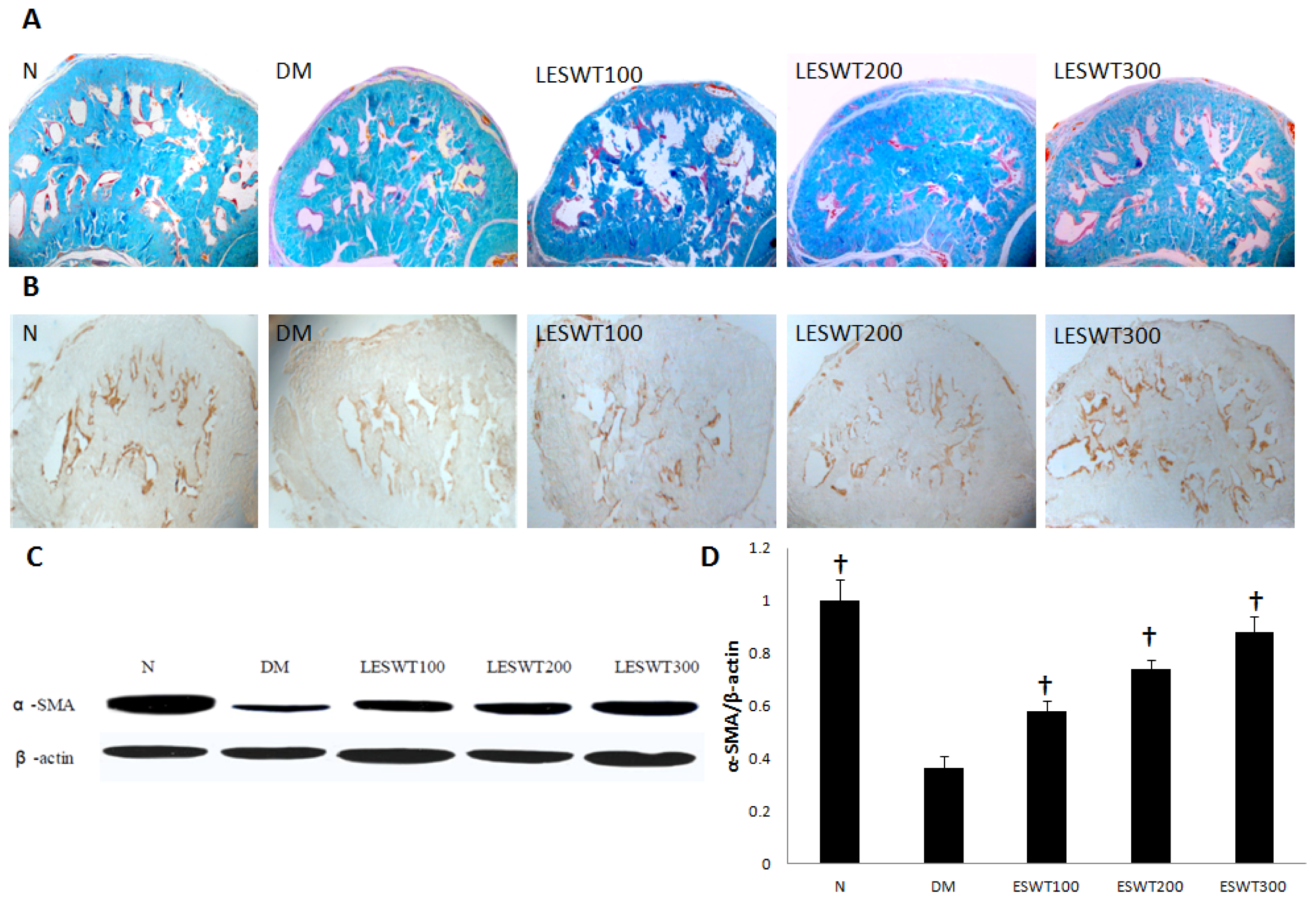
2.3. Effect of LESWT on Smooth Muscle Contents in Corpus Cavernosum
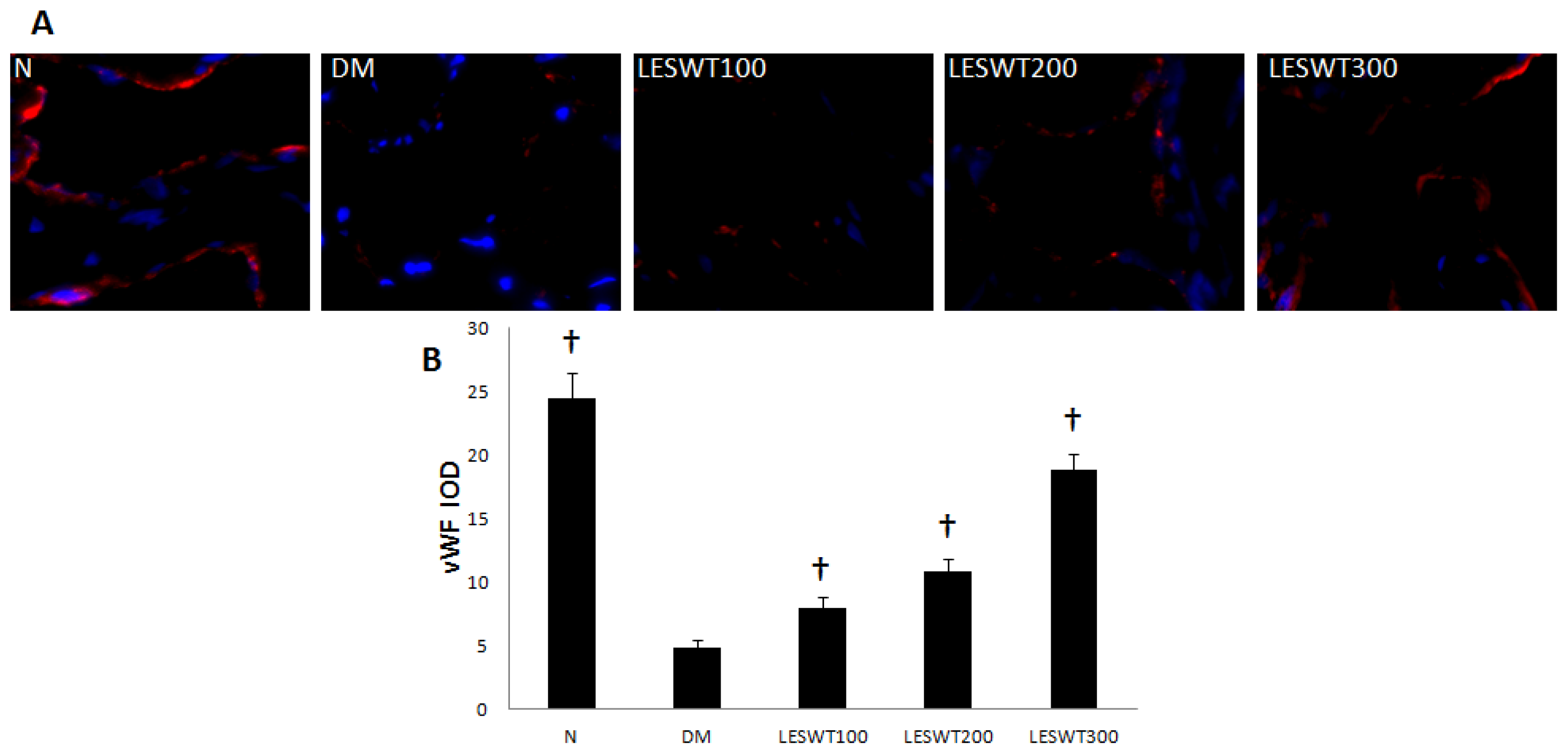
2.4. Effect of LESWT on Endothelium in Corpus Cavernosum
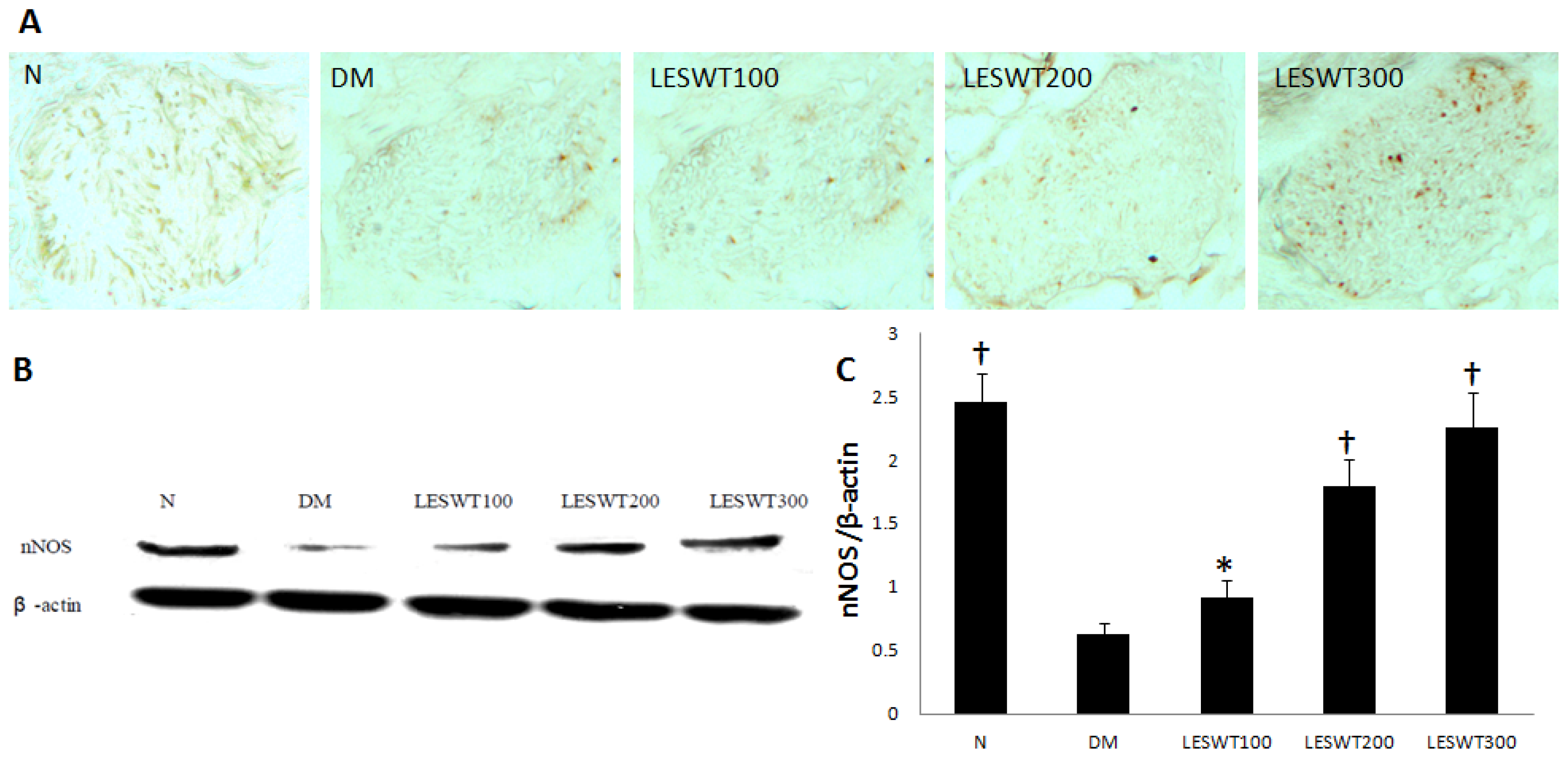
2.5. Effect of LESWT on the Expression of nNOS in Cavernous Nerve
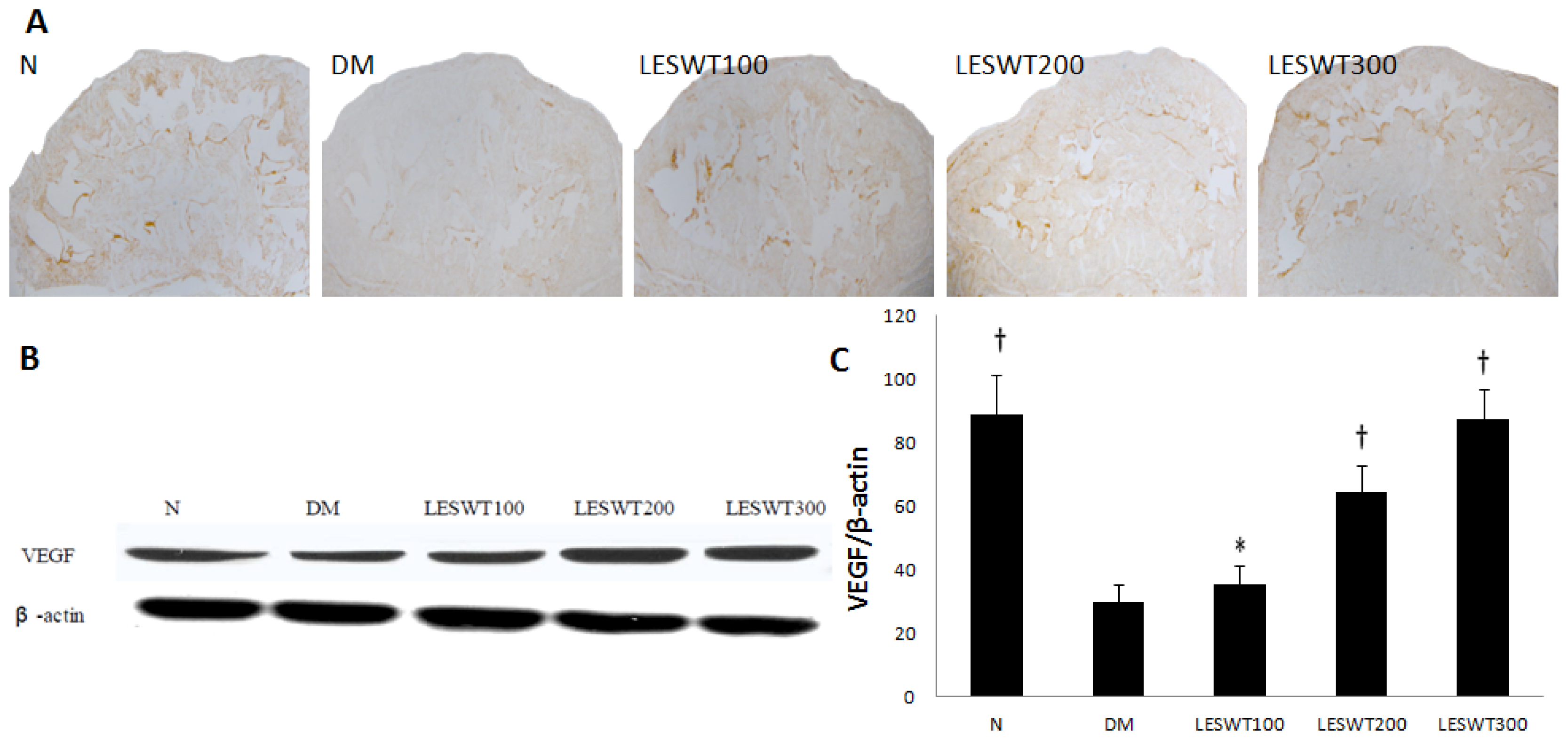
2.6. Effect of LESWT on the Expression of VEGF in Corpus Cavernosum
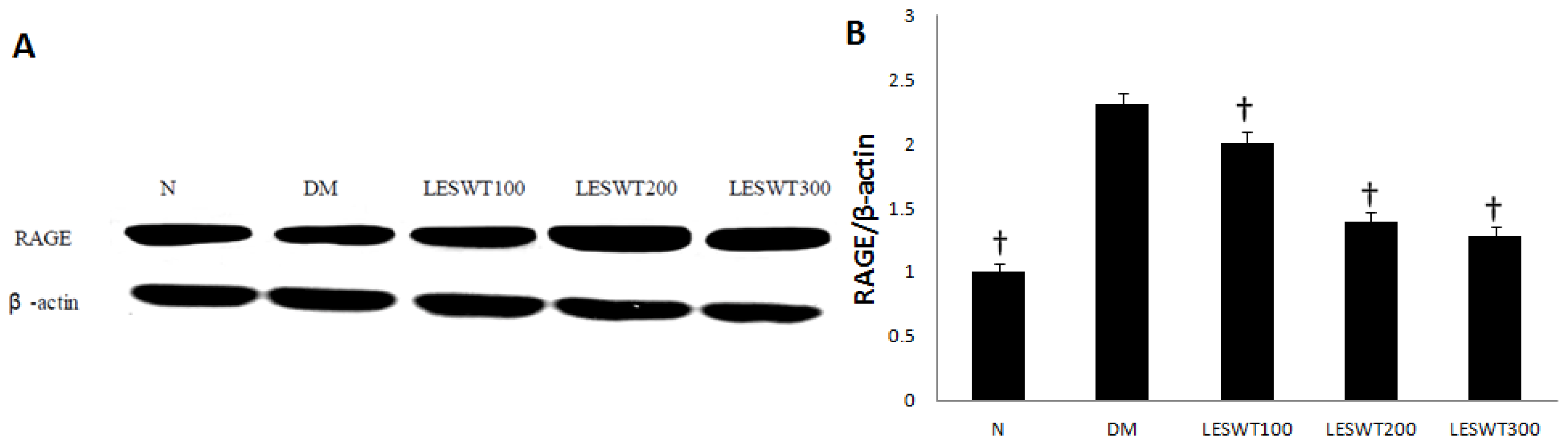
2.7. Effect of LESWT on the Expression of RAGE
3. Experimental Section
3.1. Animals
3.2. LESWT Treatment
3.3. Mesurement of Erectile Function
3.4. Histochemistry and Immunohistochemistry
3.5. Western Blot
3.6. Statistical Analysis
4. Conclusions
Acknowledgments
Conflict of Interest
References
- International Diabetes Federation. The Global Burden of Diabetes; IDF Diabetes Atlas, 2012, 5th ed Available online: http://www.idf.org/diabetesatlas/5e/the-global-burden (accessed on 7 January 2013).
- Hatzimouratidis, K.; Hatzichristou, D. ED and diabetes mellitus. Insulin 2009, 4, 114–122. [Google Scholar]
- Fedele, D. Therapy Insight: Sexual and bladder dysfunction associated with diabetes mellitus. Nat. Clin. Pract. Urol 2005, 2, 282–290. [Google Scholar]
- Hafez, E.S.; Hafez, S.D. ED: Anatomical parameters, etiology, diagnosis, and therapy. Arch. Androl 2005, 51, 15–31. [Google Scholar]
- Setter, S.M.; Iltz, J.L.; Fincham, J.E.; Campbell, R.K.; Baker, D.E. Phosphodiesterase 5 inhibitors for erectile dysfunction. Ann. Pharmacother 2005, 39, 1286–1295. [Google Scholar]
- Aversa, A.; Bruzziches, R.; Vitale, C.; Marazzi, G.; Francomano, D.; Barbaro, G.; Spera, G.; Rosano, G.M. Chronic sildenafil in men with diabetes and ED. Expert Opin. Drug Metab. Toxicol 2007, 3, 451–464. [Google Scholar]
- Zhou, F.; Li, G.Y.; Gao, Z.Z.; Liu, J.; Liu, T.; Li, W.R.; Cui, W.S.; Bai, G.Y.; Xin, Z.C. The TGF-β1/Smad/CTGF pathway and corpus cavernosum fibrous-muscular alterations in rats with streptozotocin- induced diabetes. J. Androl 2012, 33, 651–659. [Google Scholar]
- Jin, H.R.; Kim, W.J.; Song, J.S.; Choi, M.J.; Piao, S.; Shin, S.H.; Tumurbaatar, M.; Tuvshintur, B.; Nam, M.S.; Ryu, J.K.; et al. Functional and morphologic characterizations of the diabetic mouse corpus cavernosum: Comparison of a multiple low-dose and a single high-dose streptozotocin protocols. J. Sex. Med 2009, 12, 3289–3304. [Google Scholar]
- Yoshimura, N.; Kato, R.; Chancellor, M.B.; Nelson, J.B.; Glorioso, J.C. Gene therapy as future treatment of erectile dysfunction. Expert Opin. Biol. Ther 2010, 10, 1305–1314. [Google Scholar]
- Lin, C.S.; Xin, Z.C.; Wang, Z.; Deng, C.; Huang, Y.C.; Lin, G.; Lue, T.F. Stem cell therapy for erectile dysfunction: A critical review. Stem Cells Dev 2012, 21, 343–351. [Google Scholar]
- Yasuda, I. Management of the bile duct stone: Current situation in Japan. Dig. Endosc 2010, 22, 76–83. [Google Scholar]
- Tandan, M.; Reddy, D.N. Extracorporeal shock wave lithotripsy for pancreatic and large common bile duct stones. World J. Gastroenterol 2011, 17, 4365–4371. [Google Scholar]
- Capaccio, P.; Torretta, S.; Pignataro, L. Extracorporeal lithotripsy techniques for salivary stones. Otolaryngol. Clin. North Am 2009, 42, 1139–1159. [Google Scholar]
- West, D.L.; Hawuins, B.J.; Langerman, R.J. The use of extracorporeal shock waves in the treatment of delayed unions and nonunions. Curr. Orthop. Pract 2008, 19, 218–222. [Google Scholar]
- Furia, J.P.; Rompe, J.D. Extracorporeal shock wave therapy in the treatment of chronic plantar fasciitis and Achillestendin opathy. Curr. Opin. Orthop 2007, 18, 102–111. [Google Scholar]
- Gutersohn, A.; Gaspari, G. Shock waves upregulate vascular endothelial growth factor m-RNA in human umbilical vascular endotheliums. Circulation 2000, 102, 1–18. [Google Scholar]
- Wang, C.J. An overview of shock wave therapy in musculoskeletal disorders. Chang Gung Med. J 2003, 26, 220–232. [Google Scholar]
- Kenta, I.; Yoshihiro, F.; Hiroaki, S. Extracorporeal shock wave therapy as a new and non-invasive angiogenic strategy. Tohoku J. Exp. Med 2009, 219, 1–9. [Google Scholar]
- Chitale, S.; Morsey, M.; Swift, L.; Sethia, K. Limited shock wave therapy vs. sham treatment in men with Peyronie’s disease: Results of a prospective randomized controlled double-blind trial. BJU Int 2010, 106, 1352–1358. [Google Scholar]
- Goertz, O.; Lauer, H.; Hirsch, T.; Ring, A.; Lehnhardt, M.; Langer, S.; Steinau, H.U.; Hauser, J. Extracorporeal shock waves improve angiogenesis after full thickness burn. Burns 2012, 38, 1010–1018. [Google Scholar]
- Fiorenzo, A.; Christoph, K.; Axel, V. Can cellulite be treated with low-energy extracorporeal shock wave therapy? Clin. Interv. Aging 2007, 2, 623–630. [Google Scholar]
- Vardi, Y.; Appel, B.; Jacob, G.; Massarwi, O.; Gruenwald, I. Can Low-dose extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic ED. Eur. Urol 2010, 58, 243–250. [Google Scholar]
- Hatzimouratidis, K. Can we cure ED? Eur. Urol 2010, 58, 249–250. [Google Scholar]
- Vardi, Y.; Appel, B.; Kilchevsky, A.; Gruenwald, I. Does low dose extracorporeal shock wave therapy have a physiological effect on erectile function? Short-term results of a randomized, double-blind, sham controlled study. J. Urol 2012, 187, 1769–1775. [Google Scholar]
- Szkudelski, T. Streptozotocin-nicotinamide-induced diabetes in the rat. Characteristics of the experimental model. Exp. Biol. Med 2012, 237, 481–490. [Google Scholar]
- Hsieh, C.H.; Liu, S.P.; Hsu, G.L.; Chen, H.S.; Molodysky, E.; Chen, Y.H.; Yu, H.J. Advances in understanding of mammalian penile evolution, human penile anatomy and human erection physiology: Clinical implications for physicians and surgeons. Med. Sci. Monit 2012, 18, 118–125. [Google Scholar]
- Kovanecz, I.; Nolazco, G.; Ferrini, M.G.; Toblli, J.E.; Heydarkhan, S.; Vernet, D.; Rajfer, J.; Gonzalez-Cadavid, N.F. Early onset of fibrosis within the arterial media in a rat model of type 2 diabetes mellitus with erectile dysfunction. BJU Int 2009, 103, 1396–1404. [Google Scholar]
- Petschnik, A.E.; Fell, B.; Kruse, C.; Danner, S. The role of alpha-smooth muscle actin in myogenic differentiation of human glandular stem cells and their potential for smooth muscle cell replacement therapies. Expert Opin. Biol. Ther 2010, 10, 853–861. [Google Scholar]
- Vischer, U.M. Von Willebrand factor, endothelial dysfunction, and cardiovascular disease. J. Thromb. Haemost 2006, 4, 1186–1193. [Google Scholar]
- Förstermann, U.; Sessa, W.C. Nitric oxide synthases: Regulation and function. Eur. Heart J 2012, 33, 829–837. [Google Scholar]
- Ferrara, N.; Gerber, H.P.; LeCouter, J. The biology of VEGF and its receptors. Nat. Med 2003, 9, 669–676. [Google Scholar]
- Ito, K.; Fukumoto, Y.; Shimokawa, H. Extracorporeal shock wave therapy for ischemic cardio-vascular disorders. Am. J. Cardiovasc. Drugs 2011, 11, 295–302. [Google Scholar]
- Qiu, X.; Lin, G.; Xin, Z.; Ferretti, L.; Zhang, H.; Lue, T.F.; Lin, C.S. Effect of low-energy shockwave therapy on the erectile function and tissue of a diabetic rat model. J. Sex. Med 2013, 10, 738–746. [Google Scholar]
- Ramasamy, R.; Yan, S.F.; Schmidt, A.M. Receptor for AGE (RAGE): Signaling mechanisms in the pathogenesis of diabetes and its complications. Ann. N. Y. Acad. Sci 2011, 1243, 88–102. [Google Scholar]







© 2013 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Liu, J.; Zhou, F.; Li, G.-Y.; Wang, L.; Li, H.-X.; Bai, G.-Y.; Guan, R.-L.; Xu, Y.-D.; Gao, Z.-Z.; Tian, W.-J.; et al. Evaluation of the Effect of Different Doses of Low Energy Shock Wave Therapy on the Erectile Function of Streptozotocin (STZ)-Induced Diabetic Rats. Int. J. Mol. Sci. 2013, 14, 10661-10673. https://doi.org/10.3390/ijms140510661
Liu J, Zhou F, Li G-Y, Wang L, Li H-X, Bai G-Y, Guan R-L, Xu Y-D, Gao Z-Z, Tian W-J, et al. Evaluation of the Effect of Different Doses of Low Energy Shock Wave Therapy on the Erectile Function of Streptozotocin (STZ)-Induced Diabetic Rats. International Journal of Molecular Sciences. 2013; 14(5):10661-10673. https://doi.org/10.3390/ijms140510661
Chicago/Turabian StyleLiu, Jing, Feng Zhou, Guang-Yong Li, Lin Wang, Hui-Xi Li, Guang-Yi Bai, Rui-Li Guan, Yong-De Xu, Ze-Zhu Gao, Wen-Jie Tian, and et al. 2013. "Evaluation of the Effect of Different Doses of Low Energy Shock Wave Therapy on the Erectile Function of Streptozotocin (STZ)-Induced Diabetic Rats" International Journal of Molecular Sciences 14, no. 5: 10661-10673. https://doi.org/10.3390/ijms140510661