
Combination Therapy with a JNK Inhibitor and Hepatocyte Growth Factor for Restoration of Erectile Function in a Rat Model of Cavernosal Nerve Injury: Comparison with a JNK Inhibitor Alone or Hepatocyte Growth Factor Alone


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Comparison of Improved Erectile Function Effects with Administration of a JNK Inhibitor Alone, HGF Alone, or Combined Administration of the Two Agents in a Rat CNCI Model
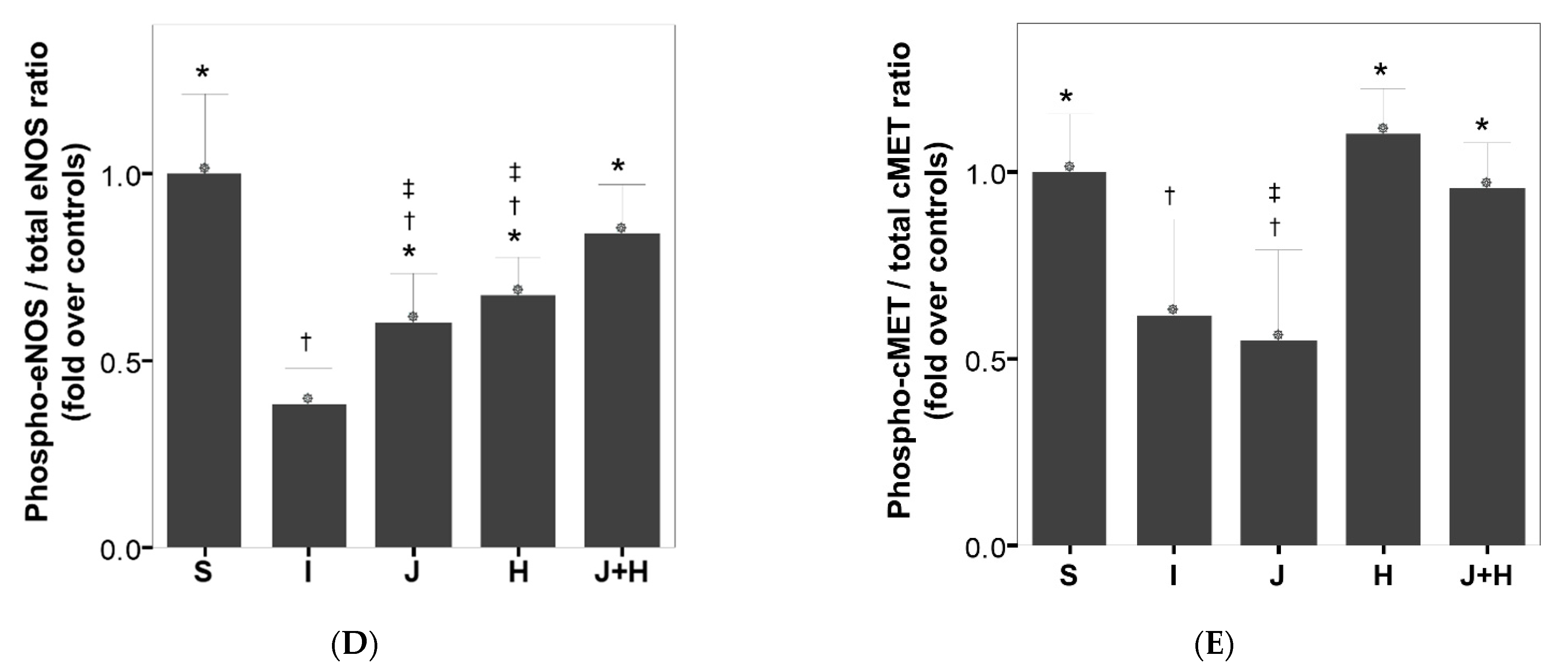
2.2. Effect of Administration of a JNK Inhibitor Alone, HGF Alone, or Combined Administration of the Two Agents on Structural and Molecular Alterations of the Cavernosal Tissues in a Rat Model of CNCI
3. Discussion
4. Materials and Methods
4.1. Experimental Animals and Study Design
4.2. Assessment of In Vivo Erectile Function and the Collection of Penile Tissues
Determination of Caspase-3 Activity
4.3. Evaluation of Structural Alterations in Corpus Cavernosum
4.4. Immunoblot Analysis
4.5. Data Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cao, L.; Yang, Z.; Qi, L.; Chen, M. Robot-assisted and laparoscopic vs open radical prostatectomy in clinically localized prostate cancer: Perioperative, functional, and oncological outcomes: A Systematic review and meta-analysis. Medicine 2019, 98, e15770. [Google Scholar] [CrossRef]
- Capogrosso, P.; Salonia, A.; Briganti, A.; Montorsi, F. Postprostatectomy Erectile Dysfunction: A Review. World J. Men’s Health 2016, 34, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.; Jung, J.H.; Jeong, C.W.; Lee, S.E.; Lee, E.; Ku, J.H.; Kim, H.H.; Kwak, C. Long-term oncologic outcomes after radical prostatectomy in clinically localized prostate cancer: 10-year follow-up in Korea. Investig. Clin. Urol. 2020, 61, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Vignozzi, L.; Filippi, S.; Morelli, A.; Marini, M.; Chavalmane, A.; Fibbi, B.; Silvestrini, E.; Mancina, R.; Carini, M.; Vannelli, G.B.; et al. Cavernous neurotomy in the rat is associated with the onset of an overt condition of hypogonadism. J. Sex. Med. 2009, 6, 1270–1283. [Google Scholar] [CrossRef]
- Mulhall, J.P. Penile rehabilitation following radical prostatectomy. Curr. Opin. Urol. 2008, 18, 613–620. [Google Scholar] [CrossRef]
- Ferrini, M.G.; Kovanecz, I.; Sanchez, S.; Umeh, C.; Rajfer, J.; Gonzalez-Cadavid, N.F. Fibrosis and loss of smooth muscle in the corpora cavernosa precede corporal veno-occlusive dysfunction (CVOD) induced by experimental cavernosal nerve damage in the rat. J. Sex. Med. 2009, 6, 415–428. [Google Scholar] [CrossRef] [Green Version]
- Philippou, Y.A.; Jung, J.H.; Steggall, M.J.; O’Driscoll, S.T.; Bakker, C.J.; Bodie, J.A.; Dahm, P. Penile rehabilitation for postprostatectomy erectile dysfunction. Cochrane Database Syst. Rev. 2018, 10, CD012414. [Google Scholar] [CrossRef]
- Mulhall, J.P.; Klein, E.A.; Slawin, K.; Henning, A.K.; Scardino, P.T. A Randomized, Double-Blind, Placebo-Controlled Trial to Assess the Utility of Tacrolimus (FK506) for the Prevention of Erectile Dysfunction Following Bilateral Nerve-Sparing Radical Prostatectomy. J. Sex. Med. 2018, 15, 1293–1299. [Google Scholar] [CrossRef]
- Chiles, K.A.; Staff, I.; Johnson-Arbor, K.; Champagne, A.; McLaughlin, T.; Graydon, R.J. A Double-Blind, Randomized Trial on the Efficacy and Safety of Hyperbaric Oxygenation Therapy in the Preservation of Erectile Function after Radical Prostatectomy. J. Urol. 2018, 199, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.D.; Milenkovic, U.; Usta, M.F.; Albersen, M.; Bivalacqua, T.J. The good, bad, and the ugly of regenerative therapies for erectile dysfunction. Transl. Androl. Urol. 2020, 9 (Suppl. 2), S252–S261. [Google Scholar] [CrossRef]
- Park, J.; Chai, J.S.; Kim, S.W.; Paick, J.S.; Cho, M.C. Inhibition of Jun N-terminal Kinase Improves Erectile Function by Alleviation of Cavernosal Apoptosis in a Rat Model of Cavernous Nerve Injury. Urology 2018, 113, 253.e9–253.e16. [Google Scholar] [CrossRef]
- Park, J.; Son, H.; Chai, J.S.; Kim, S.W.; Paick, J.S.; Cho, M.C. Chronic administration of LIMK2 inhibitors alleviates cavernosal veno-occlusive dysfunction through suppression of cavernosal fibrosis in a rat model of erectile dysfunction after cavernosal nerve injury. PLoS ONE. 2019, 14, e0213586. [Google Scholar] [CrossRef]
- Park, J.; Cho, S.Y.; Park, K.; Chai, J.S.; Son, H.; Kim, S.W.; Paick, J.-S. Role of inhibiting LIM-kinase2 in improving erectile function through suppression of corporal fibrosis in a rat model of cavernous nerve injury. Asian J. Androl. 2018, 20, 372–378. [Google Scholar] [PubMed]
- Kim, S.W.; Lee, J.; Park, J.; Chai, J.S.; Oh, S.; Paick, J.S.; Cho, M.C. Combination of LIM-kinase 2 and Jun Amino-terminal Kinase Inhibitors Improves Erectile Function in a Rat Model of Cavernous Nerve Injury. Urology 2019, 131, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.C.; Lee, J.; Park, J.; Kim, S.W. Restoration of Cavernous Veno-Occlusive Function through Chronic Administration of a Jun-Amino Terminal Kinase Inhibitor and a LIM-Kinase 2 Inhibitor by Suppressing Cavernous Apoptosis and Fibrosis in a Rat Model of Cavernous Nerve Injury: A Comparison with a Phosphodiesterase Type 5 Inhibitor. World J. Men’s Health 2020, 39, 541–549. [Google Scholar]
- Liu, R.M.; Desai, L.P. Reciprocal regulation of TGF-β and reactive oxygen species: A perverse cycle for fibrosis. Redox Biol. 2015, 6, 565–577. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.; Park, J.; Son, H.; Kim, S.W.; Paick, J.S.; Cho, M.C. Improvement of erectile function by intracavernous injection of hepatocyte growth factor in a rat model of erectile dysfunction after cavernous nerve injury. J. Sex. Med. 2018, 15, S319. [Google Scholar] [CrossRef]
- Dall’Era, J.E.; Meacham, R.B.; Mills, J.N.; Koul, S.; Carlsen, S.N.; Myers, J.B.; Koul, H.K. Vascular endothelial growth factor (VEGF) gene therapy using a nonviral gene delivery system improves erectile function in a diabetic rat model. Int. J. Impot. Res. 2008, 20, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Das, N.D.; Yin, G.N.; Choi, M.J.; Song, K.M.; Park, J.M.; Limanjaya, A.; Ghatak, K.; Minh, N.N.; Ock, J.; Park, S.H.; et al. Effectiveness of Intracavernous Delivery of Recombinant Human Hepatocyte Growth Factor on Erectile Function in the Streptozotocin-Induced Diabetic Mouse. J. Sex. Med. 2016, 13, 1618–1628. [Google Scholar] [CrossRef]
- Nakamura, Y.; Morishita, R.; Higaki, J.; Kida, I.; Aoki, M.; Moriguchi, A.; Yamada, K.; Hayashi, S.; Yo, Y.; Nakano, H.; et al. Hepatocyte growth factor is a novel member of the endothelium-specific growth factors: Additive stimulatory effect of hepatocyte growth factor with basic fibroblast growth factor but not with vascular endothelial growth factor. J. Hypertens. 1996, 14, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Sala, V.; Gatti, S.; Crepaldi, T. Cellular and molecular mechanisms of HGF/Met in the cardiovascular system. Clin. Sci. 2015, 129, 1173–1193. [Google Scholar] [CrossRef]
- Sakai, K.; Aoki, S.; Matsumoto, K. Hepatocyte growth factor and Met in drug discovery. J. Biochem. 2015, 157, 271–284. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.B.; Cho, M.C.; Paick, J.S.; Kim, S.W. Is it possible to recover erectile function spontaneously after cavernous nerve injury? Time-dependent structural and functional changes in corpus cavernosum following cavernous nerve injury in rats. World J. Men’s Health 2012, 30, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Bond, C.W.; Angeloni, N.L.; Harrington, D.A.; Stupp, S.I.; McKenna, K.E.; Podlasek, C.A. Peptide amphiphile nanofiber delivery of sonic hedgehog protein to reduce smooth muscle apoptosis in the penis after cavernous nerve resection. J. Sex. Med. 2011, 8, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Hannan, J.L.; Albersen, M.; Kutlu, O.; Gratzke, C.; Stief, C.G.; Burnett, A.L.; Lysiak, J.J.; Hedlund, P.; Bivalacqua, T.J. Inhibition of Rho-kinase improves erectile function, increases nitric oxide signaling and decreases penile apoptosis in a rat model of cavernous nerve injury. J. Urol. 2013, 189, 1155–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lysiak, J.J.; Yang, S.K.; Klausner, A.P.; Son, H.; Tuttle, J.B.; Steers, W.D. Tadalafil increases Akt and extracellular signal-regulated kinase 1/2 activation, and prevents apoptotic cell death in the penis following denervation. J. Urol. 2008, 179, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Song, W.H.; Son, H.; Kim, S.W.; Paick, J.S.; Cho, M.C. Role of Jun amino-terminal kinase (JNK) in apoptosis of cavernosal tissue during acute phase after cavernosal nerve (CN) injury. Asian J. Androl. 2018, 20, 50–55. [Google Scholar] [PubMed]
- Dhanasekaran, D.N.; Reddy, E.P. JNK signaling in apoptosis. Oncogene 2008, 27, 6245–6251. [Google Scholar] [CrossRef] [Green Version]
- Haney, N.M.; Nguyen, H.M.T.; Honda, M.; Abdel-Mageed, A.B.; Hellstrom, W.J.G. Bilateral Cavernous Nerve Crush Injury in the Rat Model: A Comparative Review of Pharmacologic Interventions. Sex. Med. Rev. 2018, 6, 234–241. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Kim, S.W.; Cho, M.C. Combination Therapy with a JNK Inhibitor and Hepatocyte Growth Factor for Restoration of Erectile Function in a Rat Model of Cavernosal Nerve Injury: Comparison with a JNK Inhibitor Alone or Hepatocyte Growth Factor Alone. Int. J. Mol. Sci. 2021, 22, 12698. https://doi.org/10.3390/ijms222312698
Lee J, Kim SW, Cho MC. Combination Therapy with a JNK Inhibitor and Hepatocyte Growth Factor for Restoration of Erectile Function in a Rat Model of Cavernosal Nerve Injury: Comparison with a JNK Inhibitor Alone or Hepatocyte Growth Factor Alone. International Journal of Molecular Sciences. 2021; 22(23):12698. https://doi.org/10.3390/ijms222312698
Chicago/Turabian StyleLee, Junghoon, Soo Woong Kim, and Min Chul Cho. 2021. "Combination Therapy with a JNK Inhibitor and Hepatocyte Growth Factor for Restoration of Erectile Function in a Rat Model of Cavernosal Nerve Injury: Comparison with a JNK Inhibitor Alone or Hepatocyte Growth Factor Alone" International Journal of Molecular Sciences 22, no. 23: 12698. https://doi.org/10.3390/ijms222312698